The Human Atmosphere, by Walter J. Kilner, [1920], at sacred-texts.com
IF the theory that forces generated within the body give rise to conditions surrounding the body which can be seen under certain circumstances, and are known as the auras, be correct, it is reasonable to anticipate that these forces will vary and cause results varying in health and disease. In the former condition, after making due allowance for age and sex, the auras, both outer and inner, are within well defined limits very similar, all variations being due to individuality. It is extremely difficult to imagine any departure from health that can occur without in some manner influencing one or more of the auric forces, and in consequence the aura itself. If the ailment be only local, then probably there will be merely a circumscribed change in the aura; but should the patient suffer from a general disease, the whole aura is liable to become affected, but as recovery takes place, it may return to its pristine state. (See cases 18 and 48.) The alteration in the aura occasionally does not seem nearly commensurate with the severity of the illness, as many of the modifications are far too subtle to be detected by the crude methods of observation at the present time available, but it must be postulated that future and more delicate processes of investigation will disclose a greater number and variety of defects. The changes most likely to be discovered at the present time are differences in size and shape of the aura accompanied by alterations of the colour and texture.
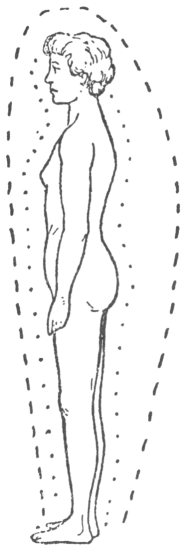
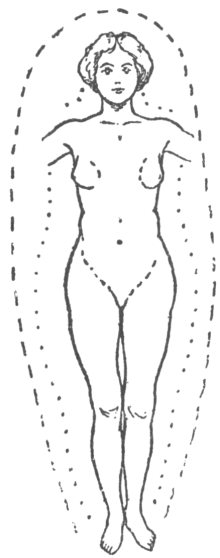
The auras of every one enjoying good health are
invariably symmetrical when they are standing facing or with their backs to the observer. One case mentioned elsewhere (case 51) is the only exception *. Down the front and the back of a person standing sideways, there is no equality. When a patient in ill health is being inspected, it is impossible, as long as the proper shape of the aura is retained, to determine whether the measurements of the aura are the same as when the patient was in good health, unless by any chance an examination either before or afterwards had taken place. (See cases 18 and 48.) It must be recollected that even it the patient had been inspected during health, a variation from the correct dimensions of his aura may be only apparent, consequent upon some change of texture, as it and visibility are closely associated.
In this chapter attention will be confined to instances in which the whole or a large portion of the aura is modified in shape from constitutional causes. The first departure from a typical aura that has been selected, is one constantly occurring, and more pronounced in women (solely on account of the natural size of the aura), than in men. In the type under consideration, the aura is symmetrical, but instead of gradually diminishing and reaching its narrowest limits not lower than the lowest part of the thighs, as in health, it suddenly contracts, almost to its fullest extent, either at the level of, or a short distance below the nethermost portion of the trunk. Using a botanical term, this shape has been named "spatulate." Seen sideways, the aura in front is of average width or even broader, while at the back there is an outward bulge in the lumbar regions. The expansion usually commences near the level of the shoulders, and contracts sharply at the same horizontal plane as at the
sides of the trunk, and then follows the contour of the body. The inner aura apparently retains the shape and size that is possessed by persons in good health.
The spatulate type of aura is strongly presumptive of a hysterical temperament, and the more pronounced the shape the more certain is the correctness of the diagnosis. Though most common in adult women, it is not confined to them, as it has been noticed in a girl eight years old, in boys of six and twelve, and in men. All these cases exhibited as perfect a spatulate aura as the natural shapes of the hazes of young girls, boys and men would permit. In every instance the mist was wider by the sides of the trunk than normal, while by the thighs it was natural in breadth or even narrow. These examples suffice to demonstrate that the hysterical form of the aura may occur in either sex. It is rarely detected in girls under the age of puberty, or in boys, nevertheless it is possible that this deviation may have been occasionally overlooked, owing to the difficulties of distinguishing characteristic alterations. It is exceedingly hard to decide whether the aura of a girl when in the transitional state, especially during the early period, is spatulate or not. Probable the intermediate stage in girls is that at which the aura usually commences taking on the abnormal form by the sides of the trunk. It is doubtful whether at birth the aura ever shows the increased breadth at the waist or the narrowing above the upper third of the thighs as is found in the typical hysterical states. In one promising case, the aura of a girl who was twelve years old and precociously developed, was carefully examined, and was found to be in the early stage of the transitional state. As she at that time displayed hysterical tendencies, it was expected that at least an abnormal bulge of the outer aura would be present in the lumbar regions at the back,
but no trace of one, and not the slightest sign of spatulate aura could be detected.
An outward curve at the small of the back seems to be present in every instance of spatulate aura. This typical bulge usually begins about the level of the shoulders, convex backwards and then curving inwards beneath the buttocks, and is almost pathognomonic of hysteria in both sexes, whilst in the male or young people it is sometimes the solitary change that can be detected.
Girls who are more emotional than normal, and who are constantly described by their relatives as "slightly hysterical," although they have never suffered seriously, show a tendency towards the spatulate aura. On the other hand women not naturally hysterical, who through grave anxiety or trouble, exhibit auras having this special feature. A well marked instance (case 35), that of a young lady will be mentioned later on.
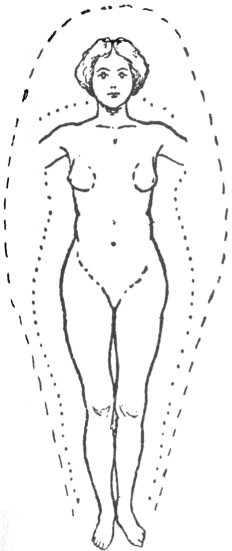
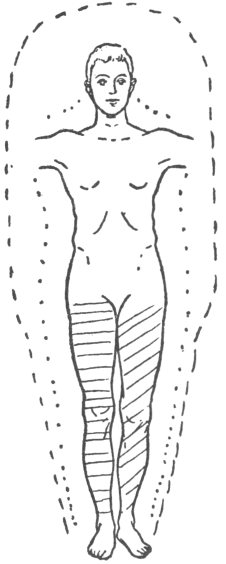
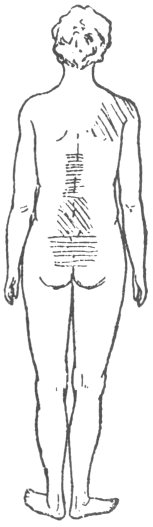
Case 29. (Figs. 29 and 30). D. X. was a girl two months under the age of seventeen years when inspected, rather tall, a perfect skeleton who five months previously had been plump. Emaciation had gradually progressed without any obvious reason, as all her organs were healthy. Menstruation, which commenced at fourteen years of age, had been in abeyance several months. She was depressed and lethargic but complained of no pain. Her family history was far from good, as she was the only child of neurotic parents. Her aura was grey tinged with a little blue, indicating a low type. Round the head the outer aura was seven inches wide, by the sides of the trunk eight, which would have been quite the average breadth for her age had not the shape been spatulate, and contracted as it reached a short distance below the lowest part of the body, where it became four and a half inches, and father decreased to three by the ankles. Sideways, it was not quite
four inches over the trunk in front and diminished down the thighs and legs; behind it was four inches at the level of the spine of the scapula, but from this point it rapidly curved outwards and again inwards regaining its former width just below the nates, and contracting slightly lower down. The greatest extent
Figs. 29 and 30.
Hysterical aura.
Spine wanting natural curves.
the bulge attained was nine inches, which in itself was remarkable for a girl of her age, especially as her spine was peculiarly straight. The inner aura was naturally striated, about three inches broad over the trunk, and a little less over the lower limbs. The colour in the interspaces between the arms and the
body, as she stood akimbo, exhibited through the different screens more yellow than was compatible with health.
Here was an ideal spatulate aura, so conspicuous that her aunt who accompanied her could easily distinguish its configuration. She was advised general massage, feeding up, etc. One visit only was paid, but her friends subsequently wrote to say that she
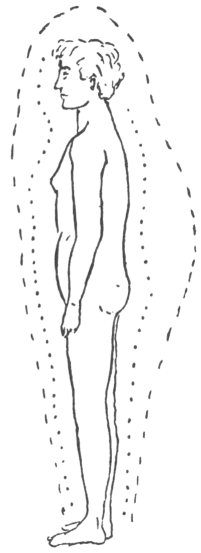
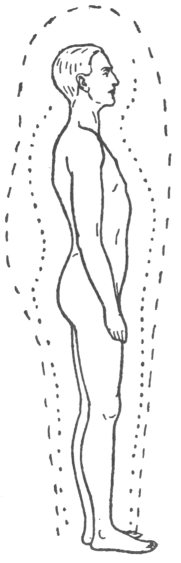
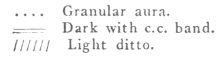
Figs. 31 and 32.
Young girl. Hysterical aura.
had regained her proper weight and appeared in good health.
Whilst examining some children for the effects of heredity upon the sizes of the aura, an early instance of the spatulate aura was discovered.
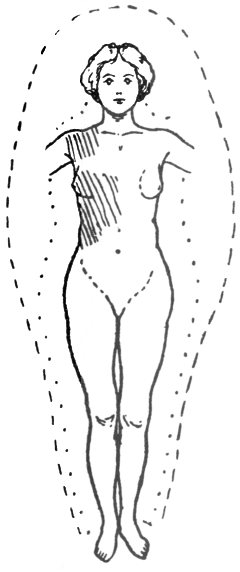
Case 30. (Figs. 31 and 32). E. X., a girl not quite eight years old was inspected in 1910. She was a bright and clever child, very excitable, but had a neurotic parentage on both sides. (See Table I.)
[paragraph continues] Her aura was bluish grey in colour. The inner was about one and a half inches wide displaying striation. On the left side over the whole of the trunk it was bright, being a good example of a pseudo-ray. (Page 52). In a short time this ray faded and the aura assumed its natural condition. There were areas of local brightness which gave the impression that rays were being emitted from various parts of the body, but none were absolutely developed. Round the head the outer aura was a little broader than the width of the shoulders. When the girl placed her hands behind her neck, the haze was four inches by the sides of the trunk, narrowing to a little less than three inches at a short distance below the pubes, from whence it proceeded regularly downwards. It was not easy to determine the exact width as the margin, especially by the lower limbs, was ill-defined. Seen sideways, the outer aura was barely three inches deep in front of the body, but at the back it bulged out, from the level of the shoulders to six inches at the lumbar region, and curved inwards a short distance below the nates. The c.c. band was even all over the body. This child had a wide aura for her age, which is all the more singular as the other members of the family had narrow ones. It was a typical specimen of an infantile spatulate aura.
Case 31. The next example has been chosen as the patient exhibited a very distinctive aura of this class. The boy was twelve years of age, far from robust, naturally quick and excitable, and had never suffered from any serious illness. His father had the same temperament, and his mother inclined to hysteria. He had been the victim of some peculiar attacks, one two years before, another about a year later, and a third a week previous to inspection. Each attack was sudden in onset, and consisted of a loss of individuality. He comprehended everything
that was taking place, but all seemed a long distance away, and quite outside his sphere of action. The attacks vanished as quickly as they came on, and afterwards he felt none the worse for them. He gave a very good account of the seizure which happened a few days before his visit. It occurred when he was at school. He knew everyone and all that was being said or done. He repeated his lessons in a parrotlike manner, but was absolutely incapable to learn anything fresh. To him, the most curious symptom was his conception of time, half an hour seeming at least three hours.
His aura exhibited a blue colour, and was seen quite easily. The outer was six and a half inches round the head, as the boy stood facing the investigator, and five inches by the sides of the trunk, being symmetrical on the two sides. It curved inwards acutely at the level of the lowest part of the trunk, where it became only three inches, and continued this breadth down the thighs and legs. Sideways, it was about three inches in front of the body, but at the back there was a bulge six inches wide, commencing at the level of the spine of the scapula, and ending at the same level as the inward curve of the aura by the sides of the trunk, and then following the usual course downwards. The inner aura was about two inches all over, and striation could be easily distinguished. The c.c. bands were even over the whole body.
The above description is so nearly the counterpart of spatulate auras in adult males, that it would be useless to quote further cases in detail.
Allied to these cases of hysteria, there are others which exhibit certain resemblances but have one important difference, viz, that they apparently develop after severe shock to the nervous system, or an injury. The name traumatic hysteria designates the complaint sufficiently well. It would be
interesting to know whether the auras of these people displayed the spatulate shape before the exciting injury occurred. Such is probably the case, although up to the present time no absolutely conclusive evidence has been obtained. It is undoubtedly instructive that one out of two or three dozen people, all of whom have met with somewhat similar accidents, should develop these nervous symptoms, while the rest remain immune from them. This fact strongly points to there being a constitutional predisposition. The youngest child whose aura displayed a perfect spatulate shape coming under this heading, was a boy six years of age. (Case 34). The early appearance of this condition after an accident, especially as it was accompanied by a rash of nervous origin, strengthens the argument for previous neurotic tendencies.
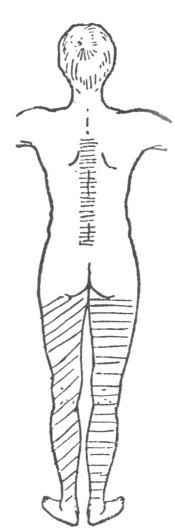
Case 32. (Figs. 33 to 35). N., a retired officer, was wounded during the South African war in the shoulder. The shock of this injury apparently induced functional heart derangement of a severe type, which necessitated a complete rest for a considerable time before he was able to return to duty. Subsequently he was invalided once or twice, and finally had to leave the army altogether. After his retirement he went from bad to worse, until at the time he came for inspection he was unable to stand without the support of a stick. Both bodily and mental exertion tired him very quickly. He had consulted many leading surgeons in London.
The outer aura nearly reached the healthy standard of distinctness, but, for a man, was extraordinarily spatulate. It was nine inches by the head, and six by the trunk, as he stood facing the observer. It curved inwards just below the level of the body, and became three inches by the legs. A side view showed it to be three inches in front, but at the back there was a bulge commencing at the shoulders and finishing
just beneath the buttocks, being at the widest part seven inches, while lower down it was only three. The inner aura was far too indistinct for health, and striation could be detected only with the greatest
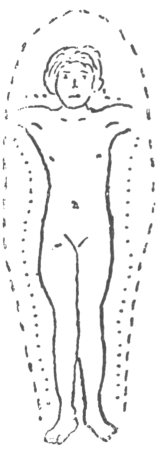
Figs. 33, 34, and 35.
Traumatic hysteria.
difficulty. It was three inches by the head and two and a half inches elsewhere.
The c.c. band was even all over the body with the exception of a long narrow patch over the spine, about two inches wide, and reaching from the fourth dorsal to the lower edge of the send lumbar vertebra. The whole of the right thigh and leg was darker than
the trunk, while the left was lighter, and the extensions beyond the limbs corresponded, being paler on the left and darker on the right. Examination had to be carried out very quickly owing to the patient's inability to stand more than a few minutes. His
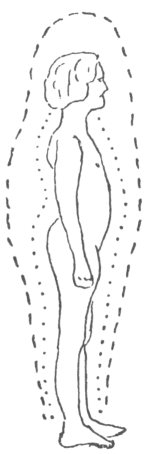
Figs. 36, 37, and 38.
Traumatic hysteria.
right leg was weaker than his left. Knee jerks were excessive and equal on the two sides.
Case 33. (Figs. 36 to 38.) D, a thin spare woman, forty-five years of age, had been a servant in one place for twenty-seven years. Her mistress considered that she was excitable, but not, as far as she knew, hysterical.
[paragraph continues] She enjoyed good health until January, 1914, the date of an accident, when she fell off a chair and hurt her back. It was expected that she would recover in a short time, but unfortunately such was not the case. She had been treated at two or three different hospitals, but became worse rather than better.
Inspection, which was made before any question was asked or any examination in the ordinary manner disclosed a spatulate aura, narrow, but of quite average distinctness. It was seven inches by the head and eight by the trunk, contracting to three by the legs. The inner aura was two and a half inches all over the body, except by the right side, where it was coarsely. granular, and appeared to be four inches in breadth. This granular portion could be seen extending round from the front to the back. Probably this apparent extra breadth of the inner aura was not genuine, but due to the outer participating in the derangement. No lineation could be detected at this place, but everywhere else it was visible. As is customary in hysterical causes, the c.c. band disclosed a good many local disturbances. There was a large multicoloured patch on the back extending from the sixth dorsal vertebra to the lower part of the sacrum. The centre portion of this patch was yellow, while the upper and lower parts were dark. On the right shoulder, both back and front, there was a yellow patch, and in front by the right side of the trunk there was another yellow patch reaching from the level of the thoracic to a short distance above the umbilical plane. The internal boundary was abrupt at the median line of the body. She complained of excessive pain in the spine and the right side of the thorax.
Case 34. A. I., a boy six years of age was examined in the early part of 1916. Until the previous July he had been healthy, rather excitable but not what
would be commonly called a nervous child. A very peculiar circumstance had frequently been noted in connection with this boy; as the result of emotion or some trivial indisposition, such as a cold, a rash would instantly break out over a portion of his body. It would be out of place to describe the rash more fully than to say it occurred in large patches and somewhat resembled Lepra Rubra. When it accompanied a cold the rash would last some hours, but if caused by excitement would vanish in from a few minutes to half an hour.
In July, 1915, he fractured his arm near the elbow joint, and was taken to a hospital, where a good deal of interest was aroused by the rash. Since the accident he had become very nervous, starting at the slightest noise, afraid of being left in the dark by himself, and incapable of doing things that he had been accustomed to do, being altogether a changed boy. Neither of his parents had shown any neurotic tendencies.
Both auras were quite plain, and the outer resembled in appearance the transitional state seen in girls of sixteen, except that it curved inwards more sharply at the level of the body. It was found to be five inches by the head and trunk, less than four by the thighs and legs, four inches in front, and at the back in the lumbar regions six and a half, being on the whole a wide aura for a boy of his age. The c.c. band was even over the whole body, with the exception of one yellow patch over the back of the neck, between the third and seventh cervical vertebræ. Query, had this patch any connection with the rash? (Compare cases 77 and 78).
Although in every instance of hysteria that has been examined the spatulate aura has been present, yet in some allied conditions where this shape has been confidently anticipated, it has been absent. The following is a remarkable example:—
Case 35. H., a young lady twenty-five years of age, when she was eighteen attended an invalid relative for a year and a half, during which time she had not a single undisturbed night's rest, although working all the day. As a consequence, after the death of her relation, she had a nervous breakdown, and from being a bright girl became dull. By nature she possessed an amiable disposition, fortunately this part of her character did not change. Outwardly she was a well formed woman, but she had an undeveloped uterus, and had only menstruated three times in her life. She had undergone an internal operation in the country, the nature of which could not be ascertained. All round her eyes the skin was deeply pigmented, of a violet hue, giving at a short distance the impression of two black eyes. When first seen she was suffering from functional hemiplegia on the right side, with almost entire loss of sensation from the clavicle downwards, and was only able to crawl a few steps without the aid of a stick. Under treatment she soon regained the use of her limbs, and sensation became normal.
One peculiarity of her case was that the affected thigh measured two inches in circumference more than the healthy one; the leg was also bigger but not to the same extent. This enlargement, due to increase of fat and not to anasarca, disappeared in a few months after her recovery, when both her lower limbs became symmetrical. A year later she had a slight relapse, which was of short duration. During her illness she was always desirous of getting well, did everything she could to help, and never showed any undue craving for sympathy.
Her aura was first inspected in January, 1909, and again in November, 1915. A description of the first examination will not be given as at that time the inner aura could not be separated from the outer. On the second occasion the outer aura was found to
be almost identical with that seen at the first examination.
The patient was in good health when inspected in 1915, but was still slow in her movements, although she seemed mentally normal. Both auras were distinct. The inner, however, hardly attained the healthy standard of clearness. It exhibited striation which could be seen without difficulty, and in breadth it reached three and a half inches by the trunk, and a little less by the limbs. The outer aura was of the ovoid type. It was nine inches and a half round the head, eleven by the trunk, and gradually contracted until it was four and a half inches by the ankles. In front it was five inches all the way down, and at the back it was four and a half inches by the shoulders, and at the widest part seven, coming down straight without any bulge. The c.c. band was even all over the body, showing no discoloured spots. Nothing unusual was seen in the colour of the aura when examined through the different screens.
Case 36. A patient lately seen possessed an extremely interesting aura, as the front view seemed normal, but the profile showed it wide in front, while at the back there was a well pronounced bulge of the hysterical type, which commenced a little below the shoulders and terminated a short distance beneath the buttocks. Reference to the diagram of a transverse section (Fig. 40, d.), will make evident the curious shape of this bulge, which was particularly prominent along the middle line.
N., a poor miserable looking woman came to be inspected in May, 1915. She was sixty-two years of age and had never been robust. Lately there had been some family trouble, and at the same time she was worrying about the war, and in consequence had a complete breakdown. Whether sitting or standing she felt that she must fall as the room was going round and round. She complained of pain in the
head, nausea, strange sensations all over the body, and inability to sleep properly. Her appearance at times was very peculiar, giving the impression that she was going out of her mind. Her mother had been insane. Upon examination no organic mischief could be found to account for the symptoms, so her ailment was considered to be pure neurasthenia. Under treatment her health rapidly improved, and she was able to leave her bed in a few days and do little things about the room. In a week or two she regained her health.
Upon inspection both auras were found to be well marked. The outer showed an approach to the spatulate type and had a huge bulge at the small of the back, beginning at the shoulders and finishing just below the nates. This part was highly characteristic of hysteria. The inner was coarsely striated, distinct, but of a most singular appearance. It seems extremely probable that the aura was in an intermediate stage between the normal and spatulate shapes.
Behind, the c.c. band disclosed two yellow patches on the back, the upper being by the left side of the spine, from the fourth to the sixth dorsal vertebræ, and the second upon the two lower lumbar vertebræ and the higher part of the sacrum, and there was a third patch on the right thigh where the patient complained of peculiar sensations. In front there was a light yellow patch over the epigastrium, due evidently to digestion, as there was no other condition to account for it. A dark spot was also seen on the lower part of the abdomen on the right side. In all these places she suffered pain and tenderness.
The colour of her aura was a bluish grey, and to the naked eye looked alike on the two sides, but the different coloured screens revealed a dissimilarity, as the right side was blue through the green screen, while the left was greenish and more opaque; through
the blue screen the inner aura on the left side was a yellow ochre, but on the right lighter and less yellow.
Besides being associated with spatulate auras, dorsal bulges occur under different circumstances. Varieties of these curves are met with in cases of organic mischief; others denote that the patient may be excitable but not necessarily neurotic. All cases of organic change of the central nervous system are attended by the dorsal curves of some description, and the absence of these is an indication against the presence of organic mischief. In one characteristic form, which may be termed "Bow-shaped," the aura usually commences to enlarge at the head and proceeding downwards attains its full width at the small of the back, and then diminishes reaching its narrowest extent not above the level of the knees, but more commonly by the ankles.
When the aura of a patient who is standing with his face or back to the observer, presents asymmetrical irregularities, the healthy side affords a good gauge for measurement and for texture, etc.; but when the patient is turned sideways, the want of a fixed unit for measurement for any increase or diminution is a serious drawback. Allowance has to be made for the variations presented by healthy subjects, and it is obligatory to fall back to a large extent upon experience, and mentally compare the aura with one known to be healthy. Speaking generally, no great trouble will be experienced when dealing with the auras of males and young girls before puberty, as they are fairly uniform all over the body. With women and girls of fourteen years and upwards the case becomes more complicated and a standard for measurement is almost essential. The best that can be devised, although open to many objections, is to take some ratio having the widest part of the aura by the sides of the trunk as the unit, in which case the breadth of the aura at the front or the back of a
patient will usually be represented by a proper fraction. In a healthy adult woman the ratio of the aura in front of the body with that of the sides is about one-third, and occasionally may be as large as one half; while the value of the dorsal aura rarely reaches two-thirds, except in neurotic females;
 Click to enlarge Fig. 39. Bow-shaped bulge. |
Case 37. (Fig. 39). B., an unmarried woman forty-six years of age, who had been unwell for a long time came to have her aura inspected. This was found to have a grey blue colour, as she stood facing, was of an average shape and size, being about eight inches by the head and trunk, and contracting to about four inches by the ankles. When she turned sideways, the outer aura made a bulge at the back commencing at the top of the head and ending at the feet, where it was four inches broad. At the widest part it was just double this width. In front it was four inches all the way down. The inner aura was narrow being only two inches wide over the whole body, very indistinct, so much so, that striation could not be defined on the right side, and was only just perceptible
on the left. The c.c. band showed a dark patch over the sixth and seventh dorsal vertebræ, a second, yellow ochre in colour, from the tenth to the twelfth dorsal vertebræ, and a third, a narrow one, on the sacrum. In front there was a patch over the right hypochondrium, dark but not so dark as those on the back. Finally the left thigh had a deeper shade all round than the right.
This patient was a school-mistress. Her illness (disseminated sclerosis), commenced, according to her own account in 1911, after an attack of influenza. She had been an in-patient at the University Hospital a short time before inspection. The disease was progressing. At the time of examination she was weak, swayed about when her eyes were closed, and had a tendency to do the same when walking. Knee jerks excessive. No nystagmus, but her pupils did not react to light or accommodation. Her left thigh and leg were wasted. She slurred her words when speaking. This, she said "she had done from a child," but a friend who accompanied her declared that the defect had increased considerably of late.
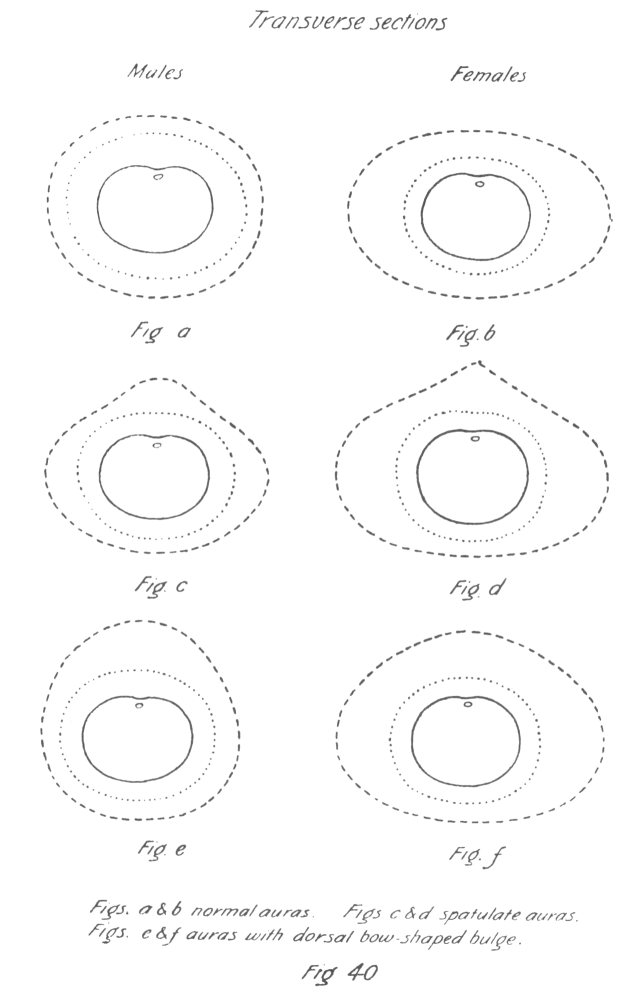
Although the aura can only be perceived for any particular position of the body as a lateral extension in the same plane, yet in health and in a considerable number of pathological states, it is not difficult to plot a diagrammatic transverse section. This has been done. Fig. 40, a and b, are those of a healthy man and woman, and the sections are supposed to be about the level of the second lumbar vertebræ. In other cases it is far from easy to draw the diagram. Take for example the spatulate aura at the waist of a patient, when the measurements are known. Here it is simple enough to make a diagram as far as the front and sides are concerned, but when it comes to the back the perplexity commences, as although the total thickness is known, yet many curves can be made from the sides of the trunk to the extreme point
Click to enlarge
Figure 40
of the aura at the back. The most likely are Fig. 40, c and e, for a man, and Fig. 40, d and f, for a woman. Personally the writer thinks that the Fig. 40, c and d, are correct for hysteria, and his opinion is founded upon a common aspect of the aura, which
Click to enlarge
Figure 40 (continued)
does not look as dense at the outer projecting part as near the body, when a patient is standing sideways; besides, the angle of the shoulders and nates, is quite as acute as has been drawn in the diagram, which makes the transverse curve somewhat similar to the vertical.
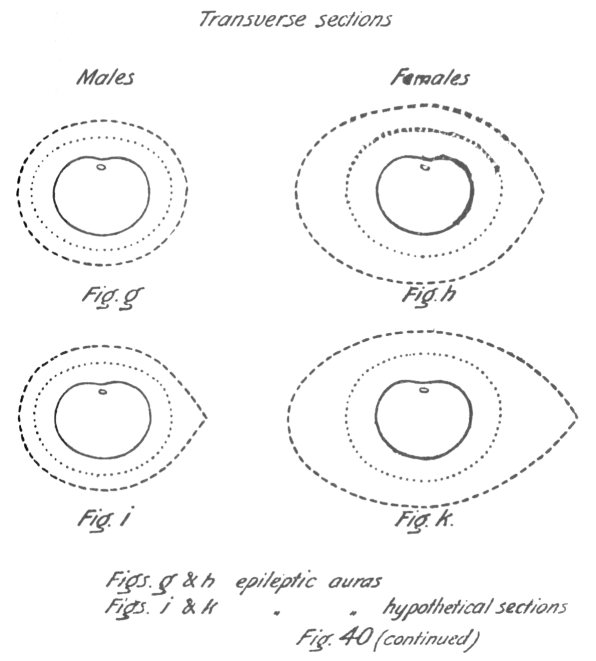
In cases where the dorsal curve commences by the head and finishes by the feet, the writer has never noticed this apparent difference of the thickness of the aura near the body and at the edge of the bulge, and consequently imagines that the shape differs from the spatulate aura in horizontal as well as in vertical sections. (Fig. 40, e and f). Of course future observations may prove this idea to be incorrect. There is a third distinct shape of the transverse section of the aura, most pronounced in epileptics, as will be seen below. (Fig. 40, g to k).
Asymmetry of the aura on two sides of the body is not a particularly uncommon occurrence, and either the outer alone or both auras may be concerned. Epilepsy, which always seems to be associated with a want of symmetry, will be taken as the first example of the asymmetrical aura.
The aura of epileptics has a complete character of its own, quite unlike the hysterical type. The latter has been just described as wide and symmetrical, while the former is peculiarly unequal. The irregularity extends from the crown of the head to the soles of the feet, and is obviously due to a contraction of the aura on one side rather than to augmentation on the other. The change is not merely one of width, but also of texture. It is singular that in every case the diminution has been on the left side, but further investigation may show that the decrease can occur on the right also. The patients who have been examined have, without exception, been right-handed, and it is highly probable that a left-handed epileptic would have his aura affected on the right side. Patients not suffering from this disease occasionally have auras simulating to some extent the typical epileptic aura. These will be considered later on, but do not in the least detract from the diagnostic value of the type in doubtful cases.
The first thing to attract the attention when the
aura of an epileptic is inspected, whether the patient has had a recent attack or not, is the marked decrease on one side of its width, and this is necessarily more conspicuous in women than in men. The observer will at once notice that the outer aura on the right side of the head is two or three inches broader than the shoulder, while on the left it
 Click to enlarge Fig. 41. Epileptic aura. |
Case 38. (Fig. 41.) N.W., a man aged forty-five years, had been strong and never had any serious illness until a few months previous to inspection, when he had an epileptic fit, and subsequently several others. None of his brothers or sisters have suffered from this complaint, nor, as far as could be ascertained, were they in any way neurotic. His children were all healthy and strong.
He has had no injury to his head to account for these attacks.
Neither aura reached the healthy standard in distinctness, as might be expected. The outer aura on the right side was clearer and wider than on the left, where it was coarser in texture. The inner aura
 Click to enlarge Fig. 42. Epileptic aura. |
Case 39. (Fig. 42.) I.E., thirty-nine years of age, had been an epileptic for over a quarter of a century, and the number of fits had gradually increased until now for months together they had been two or three
a day, and never less than three or four during the week. Her family history was bad, as her mother and sister were afflicted with the same disease, whilst the intellect of another sister was considerably below par. For the last year or two her mental powers had been failing, and she complained greatly of loss of memory. Except for the fits she had always enjoyed good health. As might be expected, her aura was typical of epilepsy. A first examination was made in 1910, and a second in 1915, the appearances on both occasions being exactly similar. The colour of her aura was decidedly below the average width for a woman. The outer was indistinct and the inner still more so, but there was no difficulty in seeing either, though their margins were ill-defined. On the left both auras were narrower, coarser and more opaque than on the right, Striation on the right could be easily observed, while on the left it remained doubtful whether any existed.
On the right side by the head and trunk the outer aura was seven inches wide, and four by the thigh and three by the leg. The breadth of the inner aura was three inches. On the left side the aura only measured five inches by the head and trunk, and by the leg three, while the inner aura was only two and a quarter inches in width. The outer aura was three and a half inches in front, four and a half at the small of the back, and three and a half by the legs. These figures show that the outer aura was narrow for a woman on the right side, and still more so on the left. The c.c. bands gave no results worth mentioning. When seen through the different coloured screens the aura did not exhibit the same hues on the two sides; the left contained more yellow.
The patient was placed upon the insulated stool and electrified, receiving several charges of positive and negative electricity alternately. The effect, though definite, was not nearly as pronounced as usual, the eventual increase being only two inches on
the right and a little less on the left, while at the same time the margins became still less marked, making it to be impossible to be sure of the exact amount of enlargement. The aura on the left side still continued to look coarser than on the right, and the comparative difference seemed to be equal, in spite of the loss of distinctness on both sides.
Case 40. X.T., a schoolboy thirteen years of age. A friend saw "the dreamy attacks," and asked his father to bring him for examination. He came in 1909, and purposely no questions were asked before inspection. The aura was obviously asymmetrical. The colour was a greenish grey. The outer aura was six inches wide by the side of the head, and the inner three inches on the right, while on the left it was four and two inches respectively. With his hands on the back of his neck, the outer aura on the right side of the trunk was four inches in breadth, narrowing about half inch lower down, and the inner was half an inch less than the outer.
On the left side the outer aura was only three inches wide, and the inner barely two and a half by the trunk, and not quite as much by the lower limbs. Sideways, the inner was about two and a half inches in breadth down the whole of the front and the outer a trifle wider. At the back the inner was the same, but the outer bulged to about six inches in the dorsolumbar region. Elsewhere it was only three inches. The c.c. band was uniform over the whole body, but the extension on the right side of the head was darker than that of the left. Strange to say there was an admixture of brown in the c.c. band beyond the body, especially on the left side. The extensions by the sides of the trunk were very similar, but the brown colour was not as well marked. When the examination was ended, his father said "that the boy was under treatment for Petit Mal, and that he never had a grave attack."
Two questions naturally arise in connection with the differences in the size of the auras on the two sides of epileptics. The first is whether the asymmetry is congenital, or whether the aura is symmetrical at birth and commences to alter with the onset of fits, and the second is whether the disparity once produced, is permanent.
There are so many difficulties in the way of determining whether the asymmetry of the epileptic aura is congenital, that it is impossible at present to arrive at a definite conclusion, but the writer is inclined to think that such is not the case.
If congenital, the shape should occur in persons who are predisposed to the malady, and it might have been expected that occasionally cases would be met with where an existing variation in the size of both the outer and inner auras on either side would point to such predisposition, although no fits had yet occurred. Up to the present time no person has been examined whose aura was suggestive of epilepsy, but undoubtedly never had a fit. When possible, the auras of near relatives of epileptics have been searched for this defect, but always with the same result.
Another important fact is, that some children who own perfectly symmetrical auras, have had convulsive seizures during the first two years of their lives. It must be remembered that it is by no means easy to examine the haze round children until about the age or six or seven years, because apart from the shyness and the difficulty of keeping them still, their auras are narrow and slight differences in size are hard to detect.
An instance (case 44), which rather militates against the theory of congenital asymmetry is that of a woman who had puerperal eclampsia. Subsequently to the seizure the auras were dissimilar on the two sides. She herself was strong and healthy before marriage, and not one of her brothers or sisters
had ever exhibited the slightest of any neurotic tendency.
If the inequalities be not congenital, they probably commence at the time of the first attack. A chance of settling this question would be afforded by observations on an individual who at first showed a normal aura, and later, after the development of epileptic seizures, manifested the typical asymmetrical alterations or no particular changes, as the case might be. It is more than likely that this point will be definitely settled in this way.
There is little or no doubt that auras which have developed typical epileptic characteristics are permanently affected, as the following example illustrates:
Case 41. B., a fresh-looking woman, thirty-nine years of age, came to have her aura inspected on account of a fall six months previously, when she injured her left shoulder, arm, and side. Pain had been continuous since the accident. If she lifted any weight she had a dragging sensation in the left side of her abdomen. She had been losing her spirits and becoming weak from the time of her accident. The observer did not expect to find any alteration in the shape of the aura, or at the very most, a slight tendency towards the spatulate type, and was quite unprepared to see the changes that were actually present.
With the patient facing, the outer aura on the right side was ten inches by. the head and trunk, and six by the leg, which was rather wide for that part. It was natural in appearance, of a grey blue colour, and its outer margin was fairly distinct. The inner aura was three inches wide and definitely striated. On the left side the outer was no more than eight inches by the head and trunk, and not quite four by the leg. It looked coarse and its edge was indistinct. The inner aura was two and three quarters inches in breadth, and roughly striated. The latter emitted a short ray
about four inches long from the injured shoulder. In order to make perfectly sure that the light did not induce disparity in size on the two sides, the patient was asked to turn completely round, but no alteration was visible. A side view showed the aura to be four inches wide in front, and the same width at the back except that there was a bulge commencing at the level of the shoulders and finishing just below the nates. Its broadest part was eight incites thick. The contraction of the aura on the left side of the head indicated that the diminution in width over the whole of the left side could not have been produced by the accident, as the injury was lower down. It is unnecessary to enter into the further details of blemishes demonstrated with the c.c. bands, etc., as they do not throw any light upon the subject under discussion.
The patient was placed upon the insulated stool and negatively electrified for five minutes. An enlargement of the outer aura developed, and as far as could be judged, was proportionately even all over, making the inequality of the outer aura still more conspicuous than before. The inner aura remained constant.
The above being a typical epileptic aura, the patient was asked immediately after the examination, whether she had ever suffered from fits, though there was nothing in her general appearance or the history she had given to suggest epilepsy. Without a moment's hesitation the answer was, "that she had had no fits since she was twelve years old, but previous to that age for two or three years, she had had two or three a year, and she believed also that she had suffered from infantile convulsions."
Here was an instance of the permanence of the epileptic type of aura, although the seizures had been in abeyance for twenty-seven years. If not congenital, the asymmetry must have developed during
childhood. The writer does not think it possible that apart from the fuller history a suspicion of epilepsy would have arisen.
Case 42. In October, 1915, N.E., a woman thirty-four years of age, came to have her aura inspected. She complained of being very languid and unable to do her work properly for some time. She often fainted. These fainting attacks came on when she was standing, sitting, or lying. Sometimes she gradually lost consciousness, and at times was able to ward off an attack by voluntary efforts, and in several instances she had not known about the seizure until it was all over. Her heart was rather irritable, but there was no organic mischief. Her father had had a fit fifteen years earlier, which at the time was considered epileptic, otherwise she appeared to be the only neurotic member of a large family. It was thought that the inspection of the aura would have been a commonplace affair, and would decide whether the so-called faints were of nervous origin or clue to the general state of health. The whole aura was so different to any seen before, that a detailed description will be interesting.
The first thing to attract notice was, that the whole aura did not come up to the average in distinctness, although sufficiently clear to be easily seen and examined. The second that the external margin was extremely ill-defined, and on cursory examination the aura appeared wide on account of a very evident ultra-outer aura. After prolonged and careful investigation it was concluded that the ordinary outer aura was of average width by the trunk, but was broad by the lower part of the thighs and legs. It was estimated to be nine inches by the head and trunk, six by the legs, while a side view showed it to be six inches in front, eight at the small of the back, and six by the legs. Here the symmetry ended, as the aura, which was blue with an admixture of a little grey,
differed on the two sides, the right being of a purer colour. Further the haze was coarser on the left side than on the right. In order to make sure that there was no inequality in the lighting, etc., during any part of the inspection, the patient was requested to turn completely round several times, but no alteration could be detected. When the inner aura was examined through the red screens (several different shades of the colour were employed), on the right side it was obviously broader by quite an inch, more distinct, and more markedly striated than on the left. It was four and a half inches by the right side of the trunk, and half an inch less by the thigh and leg, and was the same width at the back and front, while over the left side it was only three inches all the way down. The c.c. bands did not make any disclosures that need be mentioned here.
The most uncommon feature of this aura was the size and clearness of the ultra-outer aura. In aspect it was about half way between the ultra-outer aura, as generally seen, and the effect of the enlargement induced by static electricity.
After a metal brush connected with the positive pole of a large Wimshurst machine had been moved up and down the spine a few times without touching, a considerable portion of the ultra-outer aura was more distinct, but it still faded away gradually until it became unrecognizable. However, it gave a decided impression that the right side was a good deal broader than the left. After the patient had been placed upon the insulated stool and charged alternately positively and negatively several times, the same condition was maintained.
With hands placed on the hips and elbows extended, the aura in the interspaces between the arms and the body, when examined through the different screens, showed dissimilar hues on the two sides, the left having a larger addition of yellow.
|
Screens. |
R |
O |
Y |
G |
B |
V |
|
Right. |
Red. |
Yellow & Blue. |
Blue. |
Blue. |
Blue. |
Blue. |
|
Left. |
Red & Blue. |
Yellow. |
Yellow. |
Yellow & Green. |
Yellow& Blue. |
Yellow & Blue. |
The dissimilarity of the aura on the two sides was further enhanced when the back was fumed with iodine. Instead of affecting the two sides equally, it made the aura on the left side a red-brown, while on the right it was only slightly altered.
In this case all the characteristics of an epileptic aura were present, except that a diminution of the outer aura on the left side could not be satisfactorily determined, on account of the ultra-outer aura, but after electrification it gave the impression of being narrower, or if not really smaller, the distal portion was more faint.
Eight months later the patient was inspected a second time. The general appearances were the same. Nothing that could assist in the explanation of the unusual features was discovered.
Case 43. A somewhat analogous case was examined in 1918. The patient, S.J., was an old soldier who had become epileptic, and attributed the fits to a blow on the head received during the South African War. Some hesitation may be felt in admitting the sufficiency of the cause assigned, as the blow was not a severe one, not even keeping him from his work, while the attacks did not commence until a long time afterwards. Lately the fits have been increasing in frequency, and there are generally several within a few hours of each other, succeeded by a lengthy interval of freedom.
Inspection showed a well marked ultra-outer aura, extremely wide for a man. The margins were so ill-defined as to make the true dimensions of the outer aura uncertain. There was a considerable difference in the appearances on the two sides, the left being coarser and more opaque than on the right. Omitting the ultra-outer portion, the outer aura looked less wide
on the left, but owing to indefiniteness of the edge the exact size could not be ascertained with accuracy. The inner aura on the left side was roughly striated and narrower than on the right, where it exhibited a more normal lineation. At the back there was a big bulge beginning just above the shoulders and ending a little below the buttocks. The different screens showed more yellow on the left side than on the right. The patient showed no surface electricity, but after having been charged negatively, his aura expanded to a greater extent than the writer had ever seen in a man.
This patient and the previous one are the only two epileptics who have displayed an ultra-outer aura, as generally this type of aura is considerably below the average in breadth.
Up to the end of 1918, only four cases which were not definitely epileptic, had upon investigation presented both outer and inner auras on the left side of the body smaller than those on the right. All these cases had brain disturbances; one was suspected of masked epilepsy; another had puerperal eclampsia; a third was a man who had just been discharged from Bethlem Hospital; and the last was a healthy woman. (Case 51.)
Case 44. Fortunately, instances of puerperal eclampsia are by no means common, so that it was a long time before an example could be obtained for inspection. This case was supplied by a friend. Mrs. S., twenty-seven years of age, mother of three children, had convulsions in the early stage of her fourth confinement, and was delivered as quickly as possible of twins. The mother made a rapid recovery, and the children were strong and healthy. She was inspected three weeks after the birth of her infants. The aura was of a bluish grey colour, and barely up to the healthy standard of distinctness, but could be easily examined. On the right side, the outer aura was
eight inches by the head and trunk, five by the thigh and three and a half by the leg. The inner was two and a half inches all the way down. On the left side, the outer aura was seven inches by the head and trunk, and lower down it contracted to three by the ankle, while the inner was two and a quarter. The outer aura on the left side was not so plain as on the right, and the margin ill-defined, making it just possible, but not probable, that it was of the same width although looking narrower. The inner aura was not as perceptible on the left side as on the right, and striation was very faint. In front the outer aura was four inches by the trunk, five by the back, and by the thighs and legs three and a half, while the inner aura was two and a half inches back and front. Both auras were more pronounced in front of the breasts and to a lesser extent before the lower part of the abdomen, from whence a ray of the second order proceeded. The c.c. band was even all over the body, except the mammæ, where it appeared to be lighter in tint. When she put one of the infants to the breast, the colour became duller. Examined through the blue screen, the aura was a dirty ochre, but it was still more muddy looking over the left side.
This was an exceedingly interesting case, as it was impossible to predict whether any changes in the aura had taken place.
Case 45. I.X., a bootmaker by trade, fifty-eight years of age. His father and uncle had both been confined in an asylum, the latter until the day of his death. The patient was always dreading the same fate. He frequently became sullen, and without reason very depressed. These attacks of depression lasted for some hours, days or even weeks at a time. They did not, however, prevent him from following his trade. He was also liable to nervous attacks, dread, etc. Some years later he committed suicide.
His aura was inspected in 1910. The colour was
grey, and coarse in texture, especially the inner aura on the left side. The outer aura was round the head seven inches wide, and four by the trunk and leg on the right side, while the inner was two and a half inches. On the left side the outer aura was five inches round the head and by the body and leg three, the inner being two. Personally the writer considered him to be epileptic long before he commenced to study the aura, and the result of the investigation strengthens that opinion.
Case 46. This is an extremely sad case of a young man of great ability, who after a distinguished school and university career, when working for a Fellowship of his College, suddenly collapsed. He was placed in Bethlem Hospital, where he remained six months. A short time after leaving the hospital, his aura was inspected. At the time he looked dull and peculiar, and answered questions quite correctly, but slowly. He said, "he could study for an hour or two a day." The auras had the usual distinctness, were of a nondescript colour, showing blue and green without their blending. The outer aura round the head was eight inches on the right, against six on the left; four and a half inches on the right side of the trunk, and half an inch less by the thigh and leg; but on the left it was three and a half inches all the way down. The inner was two inches wide by the whole of the left side, and two and a half by the right. It showed striation everywhere, except over the right side of the head, where it was granular. The c.c. bands were even all over the body, but the right extension was darker than the left. The most conspicuous changes in the aura were concerned with its colour as seen through the different screens. The colours were so mixed without any actual blending, as to make it impossible to give an accurate description, and their distribution was also peculiar. Right side, when the red, orange, yellow, and green screens were employed, the auric
colours looked as if they were mixed with an opaque white, which was absent with the blue and violet screens, and also on the left side. Above the shoulder, with the orange screen, the aura looked blue and more distinct than by the trunk; with the green the hue was an even blue all down the body; but with the blue and violet screens, the aura showed green and yellow, and was more intense by the trunk than by the head. Left side: through the orange, yellow, and green screens, the colour of the aura was blue and yellow, the latter colour being more pronounced by the body than by the head. With the blue and the violet screens the hue was more marked by the head, being a greenish blue, but there was an addition of yellow by the side of the body.
At times the outer aura is found to be unequal on the two sides while the inner aura remains symmetrical, but this does not preclude great alterations in the latter as regards colour, texture, etc. While the inner remains normal the patient may be in good health bodily, but mentally not quite sound, as the following example will show.
Case 47. In this instance the patient has been under observation for many years, making it more than usually interesting. N.D., in April, 1907, when she was twenty years old, overworked herself at a school, teaching all the day, and studying for an examination at night. She did not retire to bed until the small hours, getting no proper sleep, as she was obliged to be up early. She went home for the Easter holidays feeling ill, and two days later developed a high temperature, the first stage of meningitis, which affected both sides of the brain. She was so ill that during one night, the nurse thought she had passed away; however, she recovered bodily, but was a changed person mentally. Instead of being rather studious and amenable to reason, she became perverse, selfish, and unable to concentrate her thoughts.
It may be interesting to note that Kernig's sign was well marked during her illness, and continued evident to a slight extent for a year and a halt, but six months later could not be detected. In September, 1908, her aura was examined. This was bluish in colour, plain, and much wider on the left than on the right side. The blue c.c. band was even over the whole body, but its extensions on the right were considerably darker than on the left side. The inspection was made before the aura could be divided into outer and inner sections.
June, 1909. Bodily health was still good and mental powers much improved. The girl had given up teaching, doing housework instead. She was able to read a little but only light literature.
In November of the same year she w as again examined. The general characters of the aura were unaltered, but the inequality had lessened. The etheric double was plainly visible on both sides, being a little over an eighth of an inch in width. The outer aura was five inches on the right against seven on the left by the head; by the trunk it was seven inches on the right and eight on the left; by the thighs and legs there was very little difference, the breadth being about four inches. The inner aura was about three inches wide and symmetrical. In profile, the outer aura was about three and a half inches in front, and another half inch at the back, while the inner was two and a half back and front.
The important point to notice was that the inner aura was alike on the two sides. Whether this would have been the case shortly after her illness must, of course, remain uncertain. Here we have an instance of partial recovery of the aura after a severe illness.
September, 1913. The patient, who for some months had been doing secretarial work, broke down again, and was obliged to give up her post. For the last few weeks severe headaches prevented her from
concentrating her mind upon work. She was very depressed, and had frequent burning sensations on the outer part of her thighs, the right being worse than the left. The same kind of discomfort sometimes attacked her right shoulder. All the pains were more acute when she was tired. There was great loss of sensation over the whole of the right thigh, and over a large patch on the abdomen, while at the back the right side was more affected than the left, and there was also a partial loss of sensation in the two feet. The strength of the right hand was perceptibly diminished, but there was no tremor. Both legs seemed equally strong. The tongue when protruded deviated to the right. The left eye was more prominent than the right, and showed internal squint but no nystagmus. Pupils reacted slowly both to accommodation and light.
Upon inspection neither aura was as distinct as in 1909, when she was in good bodily health. Although it was difficult to determine the exact size of the outer aura, there was no doubt about the right side being smaller than the left, and the inner equal on the two sides. Striation could be detected, but not easily. The c.c. band disclosed several discoloured patches on the body, all of which were tender to the touch. With arms akimbo, the aura displayed a larger amount of yellow than normal in the interspaces between the arms and trunk.
The next case is of more than ordinary interest, as it affords an example, firstly of a diminished outer aura on the whole of the right side while the inner remained unaltered in size; secondly of the quick return of the outer aura to its natural dimensions; and lastly an appearance of the outer aura almost identical with that of the ultra-outer aura, which was evidently originated by statical electricity, the effect of which persisted a long time.
Case 48. The patient was a woman thirty-seven
years of age, who had been twenty-one years in the same situation as a domestic servant. She had been in good health until three months before her inspection, when she had a severe attack of influenza, and four days afterwards began trembling. Her head and all her limbs were affected. The shaking became worse directly she tried to do anything, but ceased when lying down.
Upon examination neither aura was found to be normally distinct. The outer aura on the left side had a very perfect shape and was of average width. It was eight inches and a half by the head and trunk, six by the upper part of the thigh, and four and a half by the leg. On the right side it was narrower, being only seven inches by the head and trunk, five and four by the thigh and leg respectively, and at the same time was not as clear. The inner aura was the same size all over the body, but not so plain on the right side, where striation could be only made out with difficulty. There was a light patch over the four upper dorsal vertebræ, and by the left side of the sixth a small dark spot when the c.c. band was used. In front this band was even in colour.
In due course she was placed upon the insulated stool and negatively electrified. She, at once, complained of pain over the whole of her body. This was a very unusual occurrence as the charging rarely arouses any sensation. The machine was stopped almost immediately, but curious to relate, when she got off the stool she said "she felt brighter," and the shaking had greatly diminished. The hyperæsthesia which existed all over the body was lessened. As she thought she had benefitted she wished to be again electrified in spite of the pain. It was certain that a great improvement had taken place. This was the first case the writer had ever met with where real benefit had been derived from the action of statical electricity when applied to a patient standing upon an
insulated stool. The aura enlarged in the usual manner.
As the woman seemed so much better the writer offered to try the further effect of statical electricity. She came again on August 7th, 1917. She looked better and the tremor was considerably less. She was able to pick up a pin more easily. This time the application of electricity caused no sensation whatever. Her third visit was on the 10th of the same month, when she exhibited a marked improvement. The aura looked equal in breadth on the two sides, although there was a difference in brightness, which was less on the right. She had developed a well marked ultra-outer aura, which was evidently the result of the electrical treatment.
On the 24th she returned nearly well in health. The aura, however, continued less plain on the right side, and the patch seen by the aid of the c.c. band on the dorsal vertebræ had almost disappeared, but the ultra-outer aura remained still unaltered although she had not been electrified for a week. In order to find out the length of time this condition lasted, she was requested to come again after three weeks. This she did. The proper outline of the outer aura was distinct, but beyond the ultra-outer aura was still in evidence. There was a sharp line of demarcation between the latter and the ordinary outer aura, the two not passing gradually into one another. Probably the distal portion would have vanished in another week's time.
Case 49. (Figs. 43 and 44.) N.U., thirty-four years of age, a lady who had never been robust nor had suffered from serious illness, had lately passed through a very trying time, which had affected her health, and made her depressed and thoroughly run down. She complained of pains in her head, shoulder, and thorax en the left side. Upon examination the great occipital nerve was found to be very sensitive, and there
was a tenderness by the left side of the spine as far down as the lower dorsal vertebræ. This was especially marked at the places where the nerves emerge, and also in front at the corresponding spots on the thorax and abdomen. She was inspected for the
Figs. 43 and 44.
first time in 1908. It was noticed that the aura was considerably wider on the right side than on the left, as there were two inches by the trunk, but not so much by the head. Viewed sideways the aura was normal. The blue c.c. band was of a much lighter shade over the left side of the thorax than the right. The line of
demarcation was the median line of the body, but the change from the one side to the other was gradual. The yellow c.c. band showed a corresponding modification. In front of the abdomen the tint was even all over. When the back was examined the left side was lighter than the right, the spines of the vertebræ marking the boundary of the change.
In the following November she was again investigated after having regained fair health. As she faced the observer, it was found that the inner aura measured three inches by the side of the head and trunk, and everywhere else it was a little more than two inches. The outer aura had become symmetrical on the two sides, being eleven inches round the head, ten by the trunk and five by the legs. Sideways the outer aura was five inches in front of the body, at the small of the back seven, and down the lower limbs four inches. Although the aura was equal on the two sides, yet it exhibited a curious dissimilarity, inasmuch as the exterior margin on the right side was more sharply defined than on the left, giving the impression of being narrower.
Other changes could also be distinguished. The inner aura on the left side of the thorax, as far down as the lowest ribs, was finely granular, and more opaque than on the right. Below this level there was no difference on either side. The blue c.c. band still showed a large patch in front on the left of a lighter shade than on the right side. The demarcation lines were distinct and sharp, the upper running along the superior border of the mamma, the inner the medium line of the sternum, and the lower with the costal cartilages, and about an inch above edges. On the abdomen the band was even all over with the exception of a dark patch over the right hypochondrium, lying a little above the level of the umbilicus. On the back it was even all over, except for two small spots, one lighter in shade than the rest of the band, situated just
below the spine of the scapula on the left side, and the other darker over the sacrum. The former was tender to the touch.
Another interesting shape of the aura remains to be considered, the existence of which might have been foretold. It is characteristic of hemiplegia. In different
 Click to enlarge Fig. 45. Hemiplegia. |
Case 50. (Fig. 45.) E., a rather stout man, sixty-nine years of age, had an apoplectic fit in March, 1916. He remained unconscious for some days but had no unusual symptoms. His right arm and leg were paralysed, and he was aphasic. In a comparatively short time he regained a fair amount of power in his limbs, but his speech did not improve commensurately. He was able to understand what was said to him, but his answers were incongruous as he could rarely utter the words he wanted.
In August his aura was inspected. The outer on the right side of his head was nine inches wide, while on the left it only reached six and a half. By the trunk on the right side it was about four and a halt inches, diminishing to about three and a half by the leg. On the left side it was six and a halt by the trunk and contracted to six by the leg. Although more indistinct than it he had been in good health, on the left side the aura was still less plain than on the right,
making it extremely difficult to determine the exact width. Sideways, the aura was five inches in front, and at the back quite natural in shape, being straight down, and four inches at the shoulders and buttocks.
The whole of the inner aura was below the ordinary standard of brightness. Above the shoulders, it was massed on each side and granular, but was broader and finer on the right. On the left side it was very coarse and dense. By the same side of the trunk and leg it was three inches wide, but on the right side it was about an inch narrower. Striation could be just detected on the left but not on the right.
Examined with screens the colours were alike on the two sides, with the red, orange, and violet screens. Contrary to all expectations the hue was blue on the right, and yellow and green on the left through the green screen, while through the blue screen it was blue on the right and yellow on the left. This peculiarity, for which no explanation can be offered, is the main reason why this case has been selected as an example for hemiplegia.
A most important question arising here is whether healthy people ever have asymmetrical auras? Perhaps, it would be more to the point to ask "if the aura be not symmetrical, can a person, although apparently in good health, be so in reality, or is there present some local or constitutional defect?" Unfortunately, sufficient data are not available for arriving at a definite conclusion, because so far, only one unequivocal case that could come under this heading, has been seen. This instance occurred before the aura could be divided into the outer and inner, and consequently loses much of its interest. A careful search is made whenever an opportunity presents itself, so that this peculiarity must be far from common. It has, however, to be borne in mind that a slight difference in the size of the aura on the two sides is difficult to distinguish, especially in males and young girls
before puberty, and the detection is not made easier should, as sometimes occurs, when a person is not in good health, the outline of the aura on one side be less distinct than the other. Accordingly this investigation has had to be restricted to a great extent to women.
Case 51. C.N. was a tall and healthy woman twenty-nine years of age, whose only serious illness had been an ulcer of the stomach some few years previously. She was inspected in 1908. Her aura appeared as a light blue mist, broad by the trunk and coming down to the lower part of her thighs before it finally contracted to follow the outline of the body. For some unaccountable reason it looked wider on the right side, being twelve inches at the broadest part and three inches at the ankles. On the left it did not seem to exceed nine inches at the widest. As she stood sideways, it was nearly five inches in front of the body, and about three inches down the lower limbs. At the back it was broad down to the middle of the thighs, where it contracted.
The limits of the asymmetry and the shape of a transverse section of an aura showing the change must now be ascertained. Theoretically, in examples of inequality in shape, or dissimilarity in texture of the lateral halves of the aura, arising from systemic in contra-distinction to local causes, it would be natural to expect the junctions of the affected and unaffected aura to be situated along the median lines of the body, front and back. This has been found to be correct in several instances, of which two will be quoted.
Case 52. In April, 1912, an examination of the aura of K.N. was made. She was a young woman who had just reached her majority, and who had occasionally suffered from epilepsy since childhood, but had not had any fit prior to inspection for four years, and in spite of her long freedom from an attack, her aura still retained the epileptic type. It is unnecessary
to enter into details of its shape and size, further than to mention that they were typical. During the inspection of this patient the colour of the aura was at first a grey with a slight tinge of blue, similar to that seen at a previous and a subsequent examination. While the back was being investigated with the c.c. bands, the aura on the whole of the left side of the trunk suddenly, without any obvious cause, became darker than the right, the line of demarcation being the spine. The white background was replaced by a black one, and the colour of the aura on the left side was seen to be an ochre, very unlike the grey tint on the other side which remained unaltered. The dissimilarity was so marked that there was no difficulty in determining the junction of the two halves of the aura, by turning the patient to different angles against the background, when the vertical lines back and front were seen to be the limits of the two colours. Coincidently with this change of colour the aura on the left side appeared to have become coarser in texture than that on the right, yet it was impossible to decide whether the coarseness had really increased, or was an appearance due to the alteration of colour.
Case 53. R.F., a young lady, was inspected in 1914. Her intellect was quite up to the average. It was known that she had had three fits, the last being two days before she was brought for examination. After questioning her there could be no doubt that she was subject to numerous slight attacks (Petit Mal), which had escaped the notice of her friends. She was a tall well nourished girl, but her spinal curves were exaggerated. The first thing to attract attention was, that the aura had a different hue on the two sides of the body, the right being a blue with a little grey, and the left a green-grey. The want of resemblance was such as to make it quite easy to ascertain that the different colours came into contact with each other along the vertical median lines, back and front. The
outer aura on the left side of the head was seven inches and by the trunk eight, while by the leg it was only three and a half. On the right side it was eight inches by the head and ten by the trunk, and four and a half lower down. A profile view showed the outer aura to be four and a half inches in front, seven at the back, and four and a half by the legs. The inner aura was four inches wide on the right and three on the left.
There was a curious void space between the body and the inner aura at the small of the back, the widest portion being about an inch in breadth, and the length from seven to eight inches. The cause of this peculiarity could not be ascertained. As the patient stood facing, with her hands resting on her hips and her elbows extended, the aura was examined through different coloured screens, and showed a bluish grey through the red, orange, yellow, and green screens on the right side, while that on the left was a greenish grey. Through the blue screen the right was blue, and the left a blue and yellow unblended; lastly, through the violet screen the right showed violet and the left blue.
These two cases prove conclusively that in some instances, and perhaps in all, when the aura is not symmetrical the inequality starts at the median lines of the body front and back. If a hypothetical section of an epileptic aura be made transversely, the median lines must be taken as the points where the contraction of the aura commences. Fig. 40, g and h (page 180), show the shapes of the male and female epileptic auras as they usually appear. In some instances of epilepsy, as will be seen in cases 42 and 43, the aura on the contracted side has an exceedingly ill-defined margin, and occasionally gives the impression of extra width resembling in appearance an ultra-outer aura beyond the normal haze. From this circumstance and from want of sharpness of the edge, it seems just, and only just, possible, that in some
epileptics the outer aura may be equally wide on the two sides, and that on one side the aura may be so attenuated, as to produce the effect of contraction. Of this thin aura, Fig. 40, i and k, are suppositious transverse sections.
Case 54. (Fig. 46.) H., a married woman, was
Fig. 46.
Epileptic aura.
subject to fits. The first was noticed when she was two years old, and she knows that she has had seven others within the last two years. Before and after each attack she suffered from severe headaches, and the last one caused her temperature to remain high
for four days. She was a dull-looking woman, and evidently her mind had weakened.
She. was inspected in the latter half of 1915, when both auras were distinct and their colour grey. On the right side the outer aura was nine inches by the head and the same width by the trunk, and by the leg four. On the left side the aura was opaque in appearance, and coarse in texture, while the margin was not as defined as on the right. It was six inches by the head and trunk, and became three by the lower part of the thigh and leg. A side view showed the outer aura to be four inches in front, and at the small of the back seven and by the legs four. The inner aura was three inches on the right, and on the left two inches wide, being not merely narrower but considerably less plain.
The woman was placed upon the insulated stool and negatively charged, when the inner aura vanished first, and the outer massed on both sides of the trunk in the early stage, subsequently disappearing. After the charge had been dissipated, both auras soon returned, but it was quite ten minutes before expansion had reached its full extent. There was not the usual loss of distinctness, and the right aura looked natural in texture, while the left remained dense. The outer aura on the right side had increased to fourteen inches by the head and trunk, and six by the leg. On the left side it was nine inches by the head and trunk and four by the leg. On this side the margin had become more definite. To make sure that there was no inequality in the illumination, which might be the cause of disparity on the two sides, the patient was turned with her back to the observer, but no change could be detected. The inner aura did not seem altered.
These results assisted in arriving at the decision that the aura on the left side was not as large as on the right, by making the inequality even more conspicuous than it was previous to electrification.
If the outer aura be contracted on one side of the body, and the diminution begins at the median lines back and front, it will of necessity be lessened all over one side of the trunk, back and front, as well as beyond the body. Try as hard as possible, no occular demonstration of this phenomenon has been obtained, nor does there seem much chance of its ever being done, because the aura can be only perceived as a silhouette so that the wider portion precludes sharp definition of the latter.
Diminution of the aura, either when absolute or apparent only, must be produced by a lessening of the auric forces. If the decrease of these forces be merely quantitative, the aura will be only contracted or attenuated. (Fig. 40, g to k.) But it is more likely than not that changes in the auric forces involve some alteration in the character as well. This question will be discussed in the next chapter.
Seen during health the aura seems to be so symmetrical in size, shape, and texture, that the possibility of the existence of differences between the two sides might easily have escaped realization had not the question arisen as the direct consequences of the findings in certain pathological states.
The following is a résumé of the facts which seem to throw light upon the matter:—
I. Asymmetry in size. During the consideration of the haze surrounding epileptics, mention has been made that both the outer and the inner auras were broader on one side than on the other (page 182), in every instance with the exception of the two cases 42 and 43, where the equality of the outer is apparent, not real.
2. Asymmetry in texture. Accompanying the disparity in size, an alteration of the texture of the aura is usually present on the smaller side. (Page 182.) The vertical median lines, anteriorly and posteriorly, have been shown to be the two most likely positions
for the meeting of the asymmetrical auras, which are usually well defined. (Cases 52 to 54.)
3. Asymmetry in colour. Patients, even in perfect health, have occasionally been seen with colour differences on the two sides. In neurotics and people in indifferent health such differences are by no means uncommon, and whenever the lines of junction can be detected, they are the vertical median lines. Sometimes screens may be necessary to discover the difference. (Case 42.) For this purpose a blue screen is generally the most useful.
4. Asymmetry discovered by means of c.c. bands. Long before the question of the possibility of the existence of differences between the halves of a normal aura had arisen, it had often been noticed that the patches disclosed during examination with the c.c. bands were unilateral, especially in front, and when near the centre of the body sharply limited at the middle line.
5. Asymmetry of chemically induced changes. It has been frequently observed that when one side has been tinted by chemical vapours while the other side has been left in a natural state, the junctions of the two colours are at the median lines. The same happens when the aura on the two sides has been treated with different chemical agents.
Once or twice when the back had been fumigated by a gas, e.g., iodine vapour, to a very slight extent, the colours of the aura on the two sides did not correspond.
Asymmetry due to voluntary effort. Similarly, whenever changes have been initiated by voluntary effort, they have ceased at the central lines or, if they have, contrary to intention, extended to the other half of the body, they have been different in quality on either side of the middle line.
These considerations taken all together afford strong presumptive evidence that there are some differences
in the constitution of the aura on the two sides of the body of persons in good health, but that they are too delicate to demonstrate with our present means of investigation. Nevertheless, there is hope that in the near future this interesting question will be satisfactorily settled by further experiments.
(CASE 55.) The following example of delayed development is extremely interesting and instructive, as the patient, S.K., displayed an aura unlike any previously noted. The woman was twenty-two years of age, constitutionally healthy, but had been suffering a short time from anæmia, but not of a severe type. She had never menstruated, for which reason she wished to have her aura investigated. In figure she was tall, large, and strongly built, and inclined to stoutness. She was well proportioned except that her mammæ had retained their infantile form, the glands not being more pronounced than those of a child of six to eight years old. On the pubes there was a small quantity of hair, about as much as might have been expected at the approach of puberty. She seemed bright and intelligent for a woman of her age and occupation.
Before examination it was thought that any departure from the adult type would be in the direction of the form normally found amongst girls between the ages of fourteen and eighteen years. The result did not fulfil these anticipations.
The first impression received at the examination was, that the aura was broad round the head where it measured at least nine inches, while round the trunk it appeared not more than seven to seven and a half inches, and to descend straight to the ankles, consequently being rather wide by the thighs and legs. The margin, too, did not look as defined as usual. Careful inspection, however, showed the edge, just mentioned, not to be the true one, as the haze was in reality two to three inches broader by the trunk, but
not quite as distinct. In appearance this portion of the aura looked like an ordinary outer aura rather below the average in brightness, but not less plain than what often occurs when a patient is in ill health. It differed in character from the ultra-outer aura. This addition caused the aura to become almost spatulate in shape. In front and by the back, the outer aura was wider than usual, and had a bulge in the lumbar regions which commenced near the level of the shoulders and ended just beneath the nates. The inner aura, too, was wide, inordinately so, if the outer aura had only been seven inches in breadth, while it corresponded in size to what would most likely be found with an outer aura ten inches wide by the sides of the trunk.
After a negative charge of electricity, the outer aura became enlarged and took on an almost perfectly spatulate shape, and the bulge at the back became very pronounced. At the same time the difference in the two parts of the outer aura by the sides of the trunk grew less marked but did not entirely vanish. Unfortunately, the woman showed no signs of surface electricity, and so it was impossible to ascertain whether the maxima commonly found in females were present.
It would be useless attempting to draw any conclusion from a single case, but comparison between the above case and others in which bodily development was delayed is extremely interesting. Every girl so affected, with the exception of one, had a transitional aura narrower than usual at her age, and in one exceptional instance of an infantile type. Besides in every example which has been inspected from time to time the aura has been noticed to assume the transitional stage before the onset of menstruation. It has also been observed that the aura, although exceptions occur, is generally narrow when the sexual organs, after having commenced to function, temporarily
cease to do so from any cause. Thus there would have been nothing unusual had the aura in the case just related been from seven to seven and a half inches in breadth. The addition of the outer part is where the interest lies. A study of similar cases may possibly throw light upon the origin of the spatulate type in hysterical people.
162:* In the first edition of this book two cases were quoted of symmetrical auras in persons enjoying good health, but one of them had previously had an epileptic fit, which was not at the time admitted.