Click to enlarge
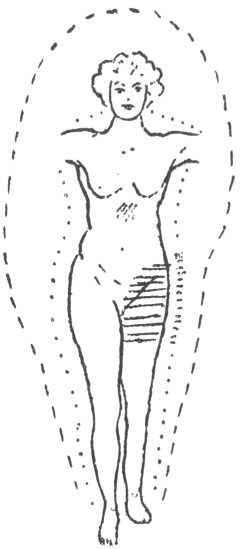
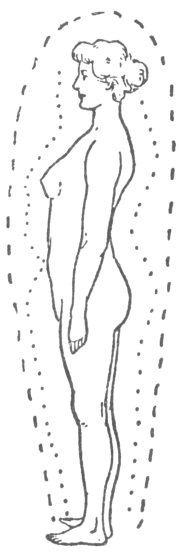
Locally contracted inner aura.
Fig. 47.
The Human Atmosphere, by Walter J. Kilner, [1920], at sacred-texts.com
IN the last chapter an account was given of the deviations of large portions of the aura from normal, and it was seen that the outer aura was affected, while the inner might or might not escape derangement. In the present chapter local changes will be considered, which will be noticed most frequently to affect the inner aura alone, though in a few cases the outer, too, is altered. In no instance, however, is there a local change of the outer without participation of the inner.
Circumscribed alterations in the shape of the aura are not so conspicuous as those described in the last chapter, and consist of either a local diminution, or occasionally of an obliteration of a part or the whole breadth of the inner aura, while external and contiguous to the deranged portion, the outer also may be to some degree affected. The inner aura besides is liable to alterations of texture, resulting in appearances completely at variance with any observed during health. The chief local modifications in structure are: (a), coarse striation of the inner aura; (b), loss of striation of the inner aura; (c), granulation of the inner aura. The last change may also affect the outer aura.
The simplest form of a local diminution is met with when a fair size of the inner aura remains in normal contact with the body, but becomes narrower from the loss of its distal portion. Usually the whole width of the impaired portion of the inner aura will be fainter, and the lineation less marked, while at the
same time the free edge will not be as sharply defined as that of the adjacent healthy areas. These changes seem to be the result of a quantitative decrease with little or perhaps no qualitative alteration of the inner auric force. The following is a typical example, which is, besides, interesting in other respects.
Click to enlarge Locally contracted inner aura. Fig. 47. |
Case 56. (Fig. 47.) X.A., a childless married woman, thirty-seven years of age, had been ill several years. Within the last four she had undergone operations for a floating kidney, double hernia, and appendicitis. As the kidney remained very moveable another operation had been suggested.
When inspected, the outer aura reached the healthy standard of distinctness. The shape was good with the exception of a wide dorsal bow, which commenced at the head and finished at the feet. The breadth was nine and a half inches round the head and by the sides of the trunk. It was six by the thighs and four and a half by the ankles. Down the front it was four and a half, while at the widest part of the bow at the back it measured nine inches. The inner aura was not quite as plain as the average, but exhibited striation all over the body. On the left side, at the front and at the back it was three inches throughout. On the right side above the level of the umbilicus, and
also from the upper third of the thigh downwards it had the same breadth, but between these two points it was only two inches wide. Here lineation was visible, inclined to be a little coarse, and the outer edge not properly defined. There was no gap between the outer and inner auras. As was expected, the c.c. band presented several discoloured areas. On the back the usual sacral patch was present, a yellow one three inches in length was perceptible above the crest of the right ilium, and a third over the right lower ribs. In front the greater part of both iliac regions was dark, but the lower part had a deeper hue than the upper. The colour was also darker on the right than on the left. There was, besides, a dark patch on the left hypochondrium. She complained of pain at each of these discoloured areas, but strange to say, both it and the tenderness were more intense in the left iliac region, although the colour here was lighter than on the right. The excessive darkening on the right side was attributed rightly or wrongly to descent of the kidney. Periodically she had acute suffering in her back, which accounted for the well marked discoloured patch.
Other variants of the contracted inner aura are the funnel-shaped and the cylindrical depressions, which often entail a complete breach of the haze. The mode of formations is probably as follows:—In chapter v., it was demonstrated that the auric forces proceed from the body in direct lines at right angles to it. If from any cause a circumscribed area be deranged in such a manner that no auric force emanates from it, while all around the affected spot the healthy parts are emitting auric force in the ordinary way, a cylindrical hollow space with its long axis at right angles to the body will be the outcome. (Case 59.) More frequently than not the deranged area, instead of being separated from the healthy portions of the body by a sharp line of demarcation, will be surrounded by zones of gradually
increasing auric forces. (Cases 57 and 58.) The result of this condition will be the formation of a conical defect, with its apex towards the body. It may be difficult to detect unless large in area, as in case 58. The effect of these void spaces in the aura upon the c.c. band has already been described.
These breaks in the inner aura can only be perceived
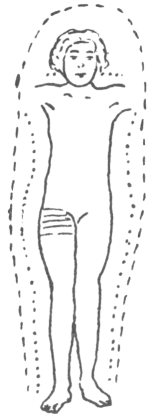
 Click to enlarge Fig 48. Funnel-shaped depression of aura. |
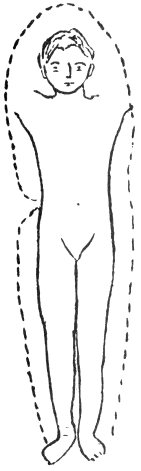
The following case occurred before the two auras could be separated, and is quoted as it was the first instance in which an aura affected by local disease was observed. As, however, the difference in size between the outer and inner auras in children is so slight, it is probable that an observation through a red screen would not have seriously affected the result.
Case 57. (Fig. 48.) H.H., a boy ten years old,
had been suffering from herpes zoster for five or six days before an opportunity of examining him presented itself. The part affected was the right lumbar region in front of the abdomen, and there were also a few spots upon the flank. The rash had reached the stage of desiccation. His aura was plainly marked, being, as he stood facing the observer, six inches by the head, and two and a half inches by the sides of the body. It was quite normal but narrow for a boy of his age, with the exception of a portion on the right side from the level of the sterno-xiphoid plane to the crest of the ilium. From the upper level just mentioned the aura curved inwards reaching the body by the twelfth rib. From this point it bent outwards, regaining its full width at the crest of the ilium. The apex of this blank space apparently touched the body, and the adjacent part of the aura did not look in any way affected either in texture or colour. Upon examination with the blue c.c. band employed transversely, the right half of the body seemed to be darker than the left, and as might be surmised, the left extension was lighter than the right. When the c.c. band was used on the back the colour was normal above the eleventh dorsal spine, but below darker, the transition between the two being abrupt. All traces of the void space vanished if the boy stood in any position except facing the observer. The aura looked perfectly normal, both at the back and front of the body.
The aura in the next case displayed a funnel-shaped depression, and when the two constituents were separated by the carmine screen the inner was seen to be more deranged.
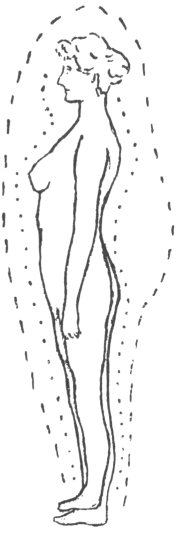
Case 58. (Fig. 49.) B., an old lady, seventy-three years of age, the mother of ten children, had been suffering for some time from pain in the epigastrium and abdomen, and coincidently losing flesh. It had been suggested that an exploratory operation would be probably required. As neither her aura nor
subsequent ordinary examination showed any definite signs of organic mischief, she was advised to wait a short time before undergoing any operation. Under treatment all pain vanished, and she regained her proper weight. Three years later she was in good health.
At the commencement of 1914, her outer aura was found to be of good shape, and
 Click to enlarge Fig. 49. Funnel-shaped depression of inner aura. |
hypochondrium. Had there been any growth it would have been beneath the dark patch, and this probably would have contained a smaller and still darker spot. Yellow patches usually indicate no serious organic mischief. It was confidently expected that the funnel-shaped depression of the inner aura would have definitely discoloured the c.c. band, but on the contrary there appeared only a small ill-defined
 Click to enlarge Fig. 50. Young girl. Hip disease. |
Case 59. (Fig. 50.) This is an extremely instructive case of a delicate looking girl, H.M., seven years of age, who in May, 1908, complained of pain in her right hip, which was diagnosed as a very early stage of tubercular hip disease. Calmette's tuberculo-ophthalmic test gave a decided reaction. As soon as possible she entered a children's hospital, where she remained an in-patient for several months, and was afterwards transferred to a convalescent home.
During February, 1909, within a day or two of her arrival home, she came to have her aura inspected. She was then looking exceedingly well, had no pain, and complete movement of her hip joint. Her aura was fairly developed, but narrow, of a greyish colour two inches wide. It was normal for a girl of her age except, that as she faced the observer, there was a complete gap two inches in length by the right trochanter major. This void space was so plainly visible and well marked that her mother noticed it immediately.
[paragraph continues] Instead of the edges curving outwards, as they did in the last case, they were quite straight, presenting a punched out appearance. The area could not be detected when she stood sideways. The c.c. band was even all over the body except where a side view exhibited a light patch over the void space.
She removed to Scotland, but in 1912, returned to London for a few weeks, when a second examination was allowed. She had grown a tall, strong, healthy girl. Her aura was a grey bluish colour, six inches wide by the head, four at the small of the back and three everywhere else. The inner aura was one and a half inches all over. Both auras looked natural for a child of her age, except round the right hip. The aura when investigated without the intervention of a screen was less distinct near the trochanter, especially close to the body. When the carmine screen was employed, the inner aura was almost completely absent at this place, and no striation could be discovered, though it was perfect above and below. The c.c. band appeared even over the whole body, back and front, except that over the right hip, it had a deeper shade, which was prolonged into the extension. Viewed sideways the band was lighter over the trochanter. Both her mother and a lady nurse who were present during the examination, were able to distinguish the abnormality without the slightest trouble.
Case 60. A woman, D.S., thirty-four years of age, had been suffering from ulcer of the stomach. She had left a hospital two months before inspection. Her complaint, which dated back five months, was her first severe illness. The outer aura, rather above the average in breadth, was a good shape and measured by the head and sides of the trunk ten and a half inches, and by the thighs six, contracting gently as it approached the ankles. A profile view showed the aura coming down straight at the back, and four inches
wide at the shoulders and nates. In front the aura ought to have been six inches in breadth before the body and lower limbs. However, there was a diminution in width from the level of the lower border of the manubrium to about the umbilical plane. This depression could not be termed funnel-shaped, but looked as if it might have been so once, and was filling up on its return to a normal condition. Here the haze was not so bright as elsewhere. The inner aura, too, was below par as regards clearness, but showed striation. The indistinctness was due to the patient not having recovered her strength. In front of the epigastrium it was narrower and fainter than over the remainder of the body, to which it was still contiguous.
The c.c. band exhibited on the back a light yellow patch by the left side of the spine from the fourth to the eighth dorsal vertebræ, and also a dark one over the two lower lumbar vertebræ and the upper part of the sacrum. In front of the body there was a patch over the epigastrium, nondescript in colour, which was more marked over the place where the pain had been previously most intense. A long dark mark running down by the rectus abdominis on the left side, and two others one in either groin, the left being deeper than the right, also came into view. In all these places the patient complained of tenderness and pain.
The different coloured screens showed no modifications, except that through the blue screen the aura looked green and yellow unblended.
The main interest in this case lay in the condition of the aura in front of the epigastrium, where a transitional stage between a void space and a healthy state had been reached, showing how the restoration of the aura takes place gradually from the body outwards.
The next change of the inner aura to be described is most difficult to understand. It consists of a diminution
in breadth at the expense of the part nearest the body, leaving an apparently vacant space between the two.
A former chapter has been devoted to the etheric double, which appears as an empty space intervening between the body and the aura. It rarely exceeds three-sixteenths of an inch in breadth, and usually passes unobserved during the inspection of a patient. Sometimes, however, when wider, it is recognized at the first glance, over the whole body, while occasionally it seems to be more clearly defined on one side than the other. The last condition is generally accompanied by some alteration of the inner aura. At times the blank space will be seen to be broadened locally, while the inner aura is proportionally narrowed with its outer margin remaining in its normal place. At present it is impossible to decide whether this vacant space is an enlarged etheric double or arises from a complete disappearance of a portion of the aura. The appearance recalls the clear space between the visible steam and the spout of the kettle from which it has issued when the water inside is boiling freely.
In well marked cases this phenomenon can hardly be missed, but in slight instances it is difficult to determine whether the gap between the body and the aura is or is not normal, and what makes it still more perplexing is, that an alteration in the texture may also be present. In many cases these empty spaces may be invisible, being obscured by the surrounding healthy aura, so probably they are really not uncommon.
No part of the body is exempt. The change has been noticed over the trunk, front, back, and sides, and upon the upper and lower limbs. It occurs most frequently in neurotic people, and also accompanies or results from various conditions, e.g., injury (case 68), growth (page 287), muscular atrophy (case 61), herpes zoster (case 62), disseminated sclerosis (case37),
etc. The duration of the change cannot usually be determined, but in a case of injury to the ribs proved to be purely temporary. (Case 68.)
In case 61 (figs. 51 and 52), an account is given of some very curious changes in the aura, including a local vacant space.
N., a woman lately married, twenty-seven years of
Figs. 51 and 52.
Old hip disease. Spatulate aura.
age, had suffered with hip disease when two years old. She had been an in-patient several times in a hospital, where she had undergone four operations, the wound of the last one only healing when she was nineteen. She was obliged to use a crutch, as her left leg was two
inches shorter, and the left thigh was four inches less in circumference than that of the right. At the time of inspection she looked a perfect picture of health.
Her aura, when examined in 1912, was blue in colour. On the right side the outer aura had a normally defined edge, and was typically spatulate, being nine inches round the head and by the trunk, curving inwards just below the lowest level of the body, becoming four inches by the knee. On the left side the aura gradually shaded off to its margin, and as far as could be verified, was eight inches by the trunk, but on a superficial examination looked less, and bent inwards at a sharp angle just below the crest of the ilium, from whence it proceeded downwards at a width of three inches. Viewed sideways, the aura was four inches in front of the trunk, the right thigh and leg, but was one inch narrower by the left thigh and leg. At the back there was the usual large lumbar bulge seen with this type of aura, being eight inches wide at the broadest part; lower down along the thighs and legs the haze had the same width as in front. The inner aura was equal in breadth over the whole body, except from the crest of the ilium to the middle of the thigh on the left side. The aura looked quite natural above the affected part, over which there appeared a dark void space three quarters of an inch deep, resembling a wide etheric double. It was impossible to determine how far round the thigh this blank space extended. External to this void the aura was coarsely striated. The outer aura here was also correspondingly coarse, and the alteration of texture was limited by the vertical median lines of the body back and front. The c.c. band was dark between the crest of the ilium and the middle of the thigh on the left side. It also disclosed a dark patch on the epigastrium due to indigestion. Otherwise the band was uniform over the whole body.
A unique phenomenon of great interest was associated
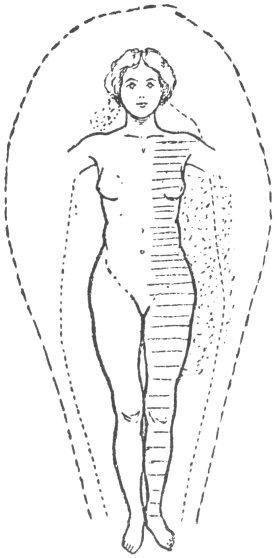
with multiple changes of the kind under consideration in a patient suffering from herpes zoster. The rash was so extensive that some derangement of the aura, short of complete absence over the entire affected area, was expected. Although the patient's aura was not very distinct, and was below the normal in clearness, the following extraordinary aspect could be easily detected:
When the patient extended his arm, the aura adjacent to the rash presented a most remarkable appearance; it seemed to be honeycombed with vacuoles beneath the arm and beside the trunk. At first the phenomenon was hard to explain, but the difficulty vanished directly it was recollected that the lines of the auric forces are at right angles to the body, and that in this instance some of them would proceed from the trunk, others from the arm, and again others from the axilla, all at different angles, causing them to be continually intersecting in the almost empty space. As the auric forces over this part of the body were, owing to the complaint, considerably below the usual strength and irregularly distributed, the haze was correspondingly small, and a cellular or spongy appearance was thus produced. This effect would also be enhanced by a more or less healthy aura at the back and in front of the pathological portion.
Case 62. F.F., a shoemaker, twenty-two years of age. When a boy of seven he had hip disease, and for years suffered from abscesses due to sequestra. He had undergone several operations, but for the last five years had enjoyed good health until a week previous to his inspection, when he noticed a rash upon the side of his chest followed by an eruption in the axilla and inner side of the arm, and another similar patch on the back accompanied by severe pain. When examined there was a herpetic patch about one and a half inches square just below the clavicle. The whole of the right axilla and three quarters of the right
arm, as well as another small place on the back near the spine at the level of the third dorsal vertebræ, were covered with the rash. The blebs were very large, some being half an inch in length. There could be no mistake about its being a severe case of herpes zoster. Inspection showed the aura to be less distinct than normal, and of a grey blue colour. On the left side it was quite natural, but very narrow, the outer being three inches in breadth and the inner two and a half. At the front and the back it was the same width, and showed no departure in shape from what would be found in health. On the right side, however, the aura was normal round the head, but as soon as the arms were raised, the appearance under the right arm and a little way down the trunk was very peculiar. It was granular but not as plainly so as usual. Against a black background, it looked as if it consisted of a haze honeycombed with dark holes. The effect produced is difficult in the extreme to describe, and the diminution of the intensity of the granular part of the aura resulted evidently from a loss of substance. Besides, the outer and inner auras appeared to be completely amalgamated, since not a vestige of differentiation could be detected. Below this disorganized portion, the aura seemed to have regained its proper condition for a short distance. Opposite the ilium, from the crest downwards, for about five inches, the haze showed a condition similar to that described, only less marked. This was contiguous to the formerly diseased joint.
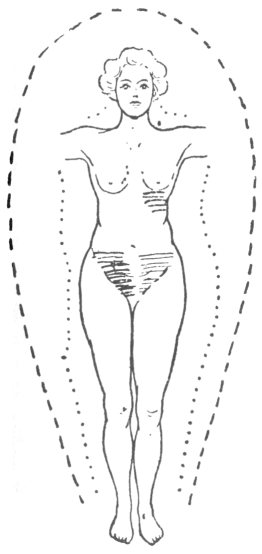
The next example is one displaying an alteration of the configuration of an aura due to local disturbance, and recovery from immediately the patient began to improve in health. Fortunately the woman allowed an examination from time to time, and thus diagrams illustrating the gradual recovery could be made. For the sake of simplicity the outer aura alone has been depicted in the diagram. Although at intervals other
cases have been seen in which auras impaired in shape have been noticed to return gradually to their natural forms, not one has shown the same amount of alteration, and none could be so closely followed.
Case 63. (Fig. 53.) D., a spinster, forty-seven years of age, whose occupation was housework, was
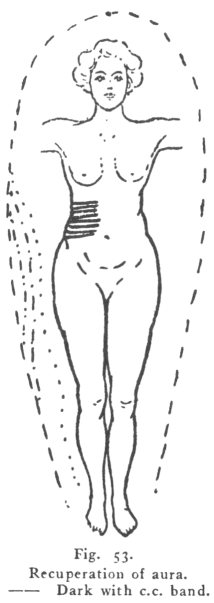 Click to enlarge Fig. 53. Recuperation of aura. |
The aura on the left side proceeded downwards in the ordinary manner for a woman, reaching the middle of the thigh before it commenced to contract permanently. It was about seven inches at the widest part. On the right it was very peculiar. Around the head it was similar to that on
the left, but at the level of the nipples, being then about six and a half inches wide, it suddenly curved inwards to a point a trifle above the level of the umbilicus, where it was only one and a half inches in breadth. From this place downwards it did not alter in width. Sideways, there was no peculiarity either at the back or in front of the body.
When the c.c. band was employed, a dark quadrilateral patch was seen over the right hypochondrium.
[paragraph continues] It started at the median line and extended round the body, having its upper edge level with the xiphoid cartilage, and its lower margin at the level of the umbilicus. This space was several shades darker than the rest of the band, and its lines of demarcation were sharply defined. Upon palpation tenderness of the liver was found, and one spot two inches above the navel and the same distance to the right of the median line, was exceedingly painful to deep pressure. The patient improved greatly under treatment.
In October, 1908, another inspection was made. The aura was unchanged except on the right side. Its curve was not so deep as formerly, and it began to widen before it finally contracted at the same level as on the left side, viz., about the middle of the thigh.
Six months later the inward curve of the aura on the right side could still be plainly seen, but had greatly diminished, otherwise there was no alteration. As the aura seemed to be gradually regaining its natural state, it was inspected once again in October, 1909. The patient had been suffering from indigestion for about six weeks, but after treatment for the last three had vastly improved. The aura had become quite symmetrical on the two sides of the body, but the previously affected area still continued to have a different aspect to any other part.
This modified portion of the aura commenced about the level of the xiphoid cartilage, and terminated a short distance above the crest of the ilium. It had a dull look and was coarse in texture, and its colour was not quite as blue as the healthy part. To the right it was bounded by streaks of a lighter shade proceeding straight from the body. These differed from the ordinary rays in their opacity. Here the inner aura was slightly narrowed, showed no striation and was coarsely granular. Elsewhere it was even all over the body, being two inches wide and was fairly lineated. The etheric double was well marked as a
dark space one eighth of an inch in breadth. This showed that while the aura had regained its proper shape, it had not resumed its natural condition. With the blue c.c. band the quadrilateral space in the hypochondriac region still was darker than the rest of the band, but the difference was not so pronounced. The extension band on the right side also remained of a darker hue than on the left, but the difference was less marked. Fig. 53 shows the gradual amendment in the aura from time to time.
Some months later, as the patient was in fair health, her aura was again inspected. The outer was natural in size all over the body, and symmetrical. However, the inner aura had not wholly regained its proper texture on the right side, as it remained coarse and opaque, but it showed signs of striation although the lines were unlike healthy ones. The upper and lower margins of the unhealthy aura were the sterno-xiphoid plane and a level a little higher than the crest of the ilium.
With the blue c.c. band the large dark patch was still in existence but had become less distinct than on the previous occasion. It was continued round to the back. The band also brought to view a well marked patch having ill-defined edges, on the left side, partially in the lumbar and partially over the iliac region. She had pain in this place on the previous day, and the spot was tender to palpation.
After a long lapse of time her aura was finally examined in the early part of 1917. There was nothing of special interest except that the aura on the right side had completely recovered its proper texture, leaving no trace of its former abnormal condition.
Local enlargements of the aura must now be considered. Such are always present in pregnancy, but only temporarily, and must be regarded as physiological. In fact, as will be seen in a later chapter, the increase in front of the breasts and abdomen constitute
one of the signs of that state. The two following instances are exceptions to the rule, because although in both the increase was similar to that occurring in pregnancy, this condition was not present.
Case 64. E., was the mother of two children, of whom the first was still born and the second two and a half years old. For some time after the birth of the latter child she had flooding and a polypus was removed in the succeeding year. Since the operation her periods had occurred at intervals of fourteen days, and were copious. She had missed three times. Her abdomen was very slightly enlarged. She had been feeling well, but far from strong. Her aura was bluish grey colour. It was nine inches by the head and the sides of the trunk, and four by the ankles. In profile the aura was five inches in front of the abdomen, but only three above and below, and by the thighs and legs four. The inner aura was two and a half inches over the whole body with the exception of the front of the abdomen, where it was wider. Pregnancy was diagnosed, but, as it turned out, incorrectly.
Case 65. N., a married childless woman. She was very nervous and depressed, as she had been growing thin for the last twelve months, and complained of vague pains in different parts of her body. Three years before inspection she had undergone an uterine operation. Her aura was blue, spatulate, seven inches and a half by the head, nine by the trunk, and not quite four by the ankles. Seen sideways, the outer aura was nine inches at the small of the back, and elsewhere four, and in front it was four all the way down, except the portion in front of the lower part of the abdomen, which was three quarters of an inch wider. The inner aura was two and a half inches all over the body, with the exception of the part in front of the abdomen, where it was three inches. Omitting this broader portion which was granular, the inner
aura was striated throughout. This want of lineation was evidence against pregnancy.
Nearly allied to this alteration in texture, which will be described almost directly, is the indistinctness of the inner or both auras simultaneously. A less defined striation of the inner aura than normal may be looked upon as presumptive evidence that the patient is not naturally robust, or is in a temporary or permanent state of ill-health. The only common exception is among women during pregnancy, when the inner, or more frequently both, auras, are decidedly more shadowy than is to be expected in good health. So numerous are these instances in which this condition of the auras occur, that diminution of visibility may be numbered among the less important signs of being enceinte.
A very good example of this condition is the next case, that of a strong, well-built, tall man who, having lumbago, took it into his head to cure it by fasting. When seen, although he had taken no food for nine days and only water to drink, declared that the felt quite fit, and that on the previous day, after attending to his bees all the morning, had been gardening the whole afternoon, doing, as he termed it, "navvy's work." When in his usual state of health, his aura would be pronounced wide, especially round his head, as his intellectual powers were considerably above the average. He was a barrister and a wrangler.
Case 66. H. G., aged forty-eight, was inspected in 1915. The outer aura was quite up to the normal in distinctness, and of a good shape. The inner was almost invisible, however, striation could be just detected. The c.c. band was uniform over the whole body, except that there was a yellow patch in front of the stomach. The patient owned to having discomfort at that place for the first time since he had commenced fasting, and attributed it to want of food. There was nothing worth mentioning about
the aura. It is interesting to note that his surface electricity was almost nil, while a month or two previously it had been unusually great.
Case 67. A lady thirty-four years of age, who had never been strong but never had any serious illness, was examined in 1913. A short time before she had complained or indigestion from which she had completely recovered. She was thin but that was natural to her. Several members of her family had died of consumption, but she had shown no signs of that complaint. She was regarded as a healthy but delicate woman. The colour of her aura was blue tinged with grey. The outer aura barely reached the average standard of distinctness, while the inner was far below, though striation could be detected with difficulty. The dimensions of the outer aura were nine inches by the sides of the trunk and round the head, four in front of the body, seven at the back, and by the lower limbs three and a half. The inner aura was two and a half inches by the head and trunk, and two by the legs. The c.c. band only revealed slight marks, one in front and one at the back. The colours of the aura when observed through the different screens were curious, but hardly worth mentioning here.
This condition is constantly met with in girls and young women when anæmic, but the aura returns to its normal brightness as they become convalescent.
Directly the outer and inner auras could be differentiated, it became reasonable to surmise that each of these at times would display alterations in size and structure. It has been incidentally noted that in a large number of instances, a variation in the size of the inner aura has been accompanied by a modification of substance, so that the two conditions may be conveniently studied together.
To understand the changes that take place in the texture of the inner aura, it must be borne in mind
that when healthy it is composed of an exceedingly fine haze, apparently made up of fine granules which by their arrangement impart a striated appearance. This aura keeps so nearly the same breadth over every part of the body, that it is probably the outcome of one and only one force emanating from the body, viz., the inner auric force. (Page 133).
Any departure from health is liable to derange this force, and to induce some change in the substance of the aura. One that can be frequently distinguished without the intervention of any screen, is the loss of natural striation. This is the earliest morbid modification of the inner aura.
As an adjunct to this want of striation, the incomparably fine granules constituting the inner aura in health, will be replaced by others more coarse and opaque. Apparently each of these large granules is formed by the coalescence of two or more small ones. The sizes of these granules vary greatly, but there is generally a predominance of one size which imparts a distinctive feature to the affected part. The granular state may be conveniently classified as fine, medium, and coarse, as the case may be. With the appearance of these granules, lineation first becomes coarse, and ultimately disappears. It would appear from the infrequency of alterations in breadth of the inner aura, that the intensity of the forces originating it is usually preserved, but what part, if any, it plays in the production of the abnormal granules is not known. When once the granular appearance is established, especially if coarse, a long time generally elapses before the aura returns to its pristine state. An example may be cited of a lady, who showed this peculiarity seven weeks after suffering from a stiff neck. After an interval of another five months her neck was again examined. When investigated in the ordinary manner there was a small deranged patch emanating from the lowest
part of the neck. This patch was about two and a half inches wide at the base, and two in height. The outer margin consisted of a number of points, one taller than the other until the highest was reached, and on the other side of the peak it fell away in the same manner. With a light carmine screen the spot looked finely granular, having been on the former occasion much coarser. When the c.c. bands were employed, the blue and the green on the right side were darker, while the yellow was even on the two sides. The change from the large to the small granules was obviously the precursor of a return to the normal.
The next case is extremely interesting as the patient was inspected during bad health—after an injury—and again when she was in perfect health. It was thus possible to determine whether the alterations in the aura were transient or permanent.
Case 68. U., a shop assistant, twenty-four years of age, who throughout her life had been healthy and strong, recently became the victim of indigestion, which under treatment soon disappeared. At the time of her inspection she was far from strong. Her outer aura was natural in shape, and of a greyish blue colour. By the sides of the head and trunk it was nine inches in breadth, six by the thighs and four by the ankles. In front it was four inches all the way down, and at the back showed a slight bulge seven inches wide, and by the thighs and legs it was three and a half inches broad.
The inner aura measured two and three-quarter inches by the body and a little less by the limbs. Natural striation could be recognized all over the body, except in the left hypochondriac region, where it had become coarsely lineated. The c.c. band showed the very common change on the sacrum, while over the epigastrium there was a large dark patch extending round the left side as far as the spine.
Two years later she became anæmic, always felt languid, and had a return of indigestion accompanied by dilatation of the stomach. While in this condition she was inspected a second time. the outer aura, with the exception of being enlarged in front of the abdomen, had not changed. The inner aura had lost considerably in clearness, and was decidedly below the average in distinctness, yet lineation could, without much difficulty, be perceived. It remained unchanged, except that it had increased in front of the trunk, from the level of the nipple line to a short distance above the umbilicus. Here striation was visible, but was coarse and had a tendency to become granular. Examination with the c.c. band disclosed a large yellow spot over the left hypochondrium.
As this enlargement of the aura was not present in front of the abdomen during the first inspection, it is evident that it could have been in existence only a comparatively short time, so it was thought that another examination would prove whether the augmentation was temporary or permanent, and thus be instructive. The woman kindly assented, but unfortunately was unable to fulfil her promise for a considerable time, as during the interval she married and her new home was in the north of England.
Her third inspection took place in the autumn of 1916, when she was still feeling the effects of a fall which resulted in two fractured ribs on the right side. It is unnecessary to enter into the details of this examination, as for the most part the auras remained the same, and there was no alteration in the enlargement in front of the abdomen, while the inner aura had regained its proper distinctness. However, near the site of the recent injury from the level of the sterno-xiphoid plane to the crest of the ilium, there was a void space about an inch and a half between the body and the inner aura. As owing to the injury
she could not be regarded in perfect health she came when feeling absolutely well.
In March, 1917, she was examined for the last time. Her outer aura looked unusually distinct and appeared larger than at the former inspections. After making all allowances for its indefinite margin, the outcome of a slight ultra-outer aura, there was no doubt about a true increase in size. The measurements were, by the head eleven inches, twelve by the trunk, six and a half by the thighs, and four by the ankles. Back and front of the trunk it was eight inches, and down the thighs and legs it was the same as by the sides. The enlargement in front of the abdomen of both auras remained constant. The inner was coarsely striated near the seat of the injury, (where also the c.c. band looked dark), otherwise it appeared healthy over the whole body, being three inches and a half wide, and a trifle narrower by the limbs. The former blank space between the body and the haze was occupied by the inner aura in the ordinary manner. The extra width of the auras in front of the abdomen in this case must now be considered a permanent feature.
As the inner auras of persons in good health are more extensive in the robust than in the constitutionally delicate, it is extremely improbable that the broader side will prove to be abnormal when asymmetry occurs. Usually there is no difficulty in coming to a decision, as some other modification on the affected side can always be detected either directly or with the c.c. band. It will be found that whenever a contraction of the inner aura exists, a corresponding change in the outer will have taken place; but the reverse does not hold good. It is worth remembering that in every instance in which a contracted inner aura has been observed over a large surface, the patient has suffered from a grave malady.
The inspection of an epileptic shows the inner aura on the left side to be narrowed, while on the right it retains its full size. The modifications do not stop here, as invariably on the left side the texture of the aura is coarse in appearance, or even granular, causing striation when distinguishable to be detected only with difficulty. This one-sided diminution of the inner aura is far more diagnostic of epilepsy than the contracted outer aura, although the latter is considerably more conspicuous and was first discovered.
The permanence of the granular state of the inner aura reaches its zenith in one place, where it almost ceases to be pathological. This is over some part of the lower lumbar and sacral regions of many women between the ages of twenty and fifty years. In some it is the lowest part of the sacrum, in others higher up, but although in every instance the median line is affected, the patch usually extends more to one side than the other. When this condition is present an unvarying tale is told, of pain, or at least discomfort, at that place in the back during the menstrual periods. The recurrence of these cycles at short intervals does not permit sufficient time for the aura to return to its natural state before a fresh onset commences, thus making the abnormal condition perpetual. Another interesting fact is, that this patch is generally more pronounced when the pain has been severe. The granular condition may as a rule be recognized by the aid of a deep carmine screen, but before this was used, dark patches had been discovered in the c.c. bands, and their cause had been a great puzzle, until the influence of local changes had been realized. It had also been noticed that this dark patch was non-existent in men, and did not appear in girls before puberty, nor in women who had passed their grand climacteric, and that it generally vanished during pregnancy unless it was
produced by a known cause such as lumbago. An additional proof of its intimate connection with menstruation was forthcoming, when on one occasion a young lady who presented not the slightest sign of any discoloured patch over the sacrum, upon being interrogated, stated, "that she had never suffered the least pain or ache in that region during her periods." At the same examination the c.c. band exhibited a small light discoloured spot, about one and a half inches in diameter over the first lumbar spine. When questioned whether there was pain or tenderness in that place, she replied that there had been none for the last fortnight, but previously she had a good deal of pain, on one occasion so acute that she had to retire to bed. This is another instance of the long time sometimes taken by the aura before a return to normal after being granular.
Besides the very crude variations in texture which are easily perceived, such as the granular conditions, there are others of a more refined nature, imperceptible to the naked eye but distinguishable by the c.c. bands. The use of these bands will form the subject of the next chapter.
Physiological enlargements of the inner aura are of two kinds. The first only persists a short time, is very great and sometimes extends beyond the limits of the outer aura; these are the rays which have already been discussed. The second is also temporary, but of longer duration; occasionally it may persist for weeks or even months. A good illustration of this condition is seen over the front of the abdomen in pregnancy.
Pathological enlargements of the inner aura do indubitably occur, as in case 68. Whenever the inner aura look broaders (broadens?—JBH) locally and the texture has not been sufficiently altered to abolish striation throughout the whole width, there can be no doubt about a real increase if present. At the same time
the outer aura will probably also show some augmentation.
In many cases the extension of the inner aura is only specious and a result of an alteration in the adjacent outer aura, consequently it is necessary to take into consideration the structure of this aura when estimating the size of the inner. During health the portion of the outer aura lying just outside the inner has larger granules than the more distant parts. The layers of the different sized granules imperceptibly graduate into one another. When a local disturbance arises in the inner aura causing it to become granular, the grains of the outer are liable to be similarly affected to a less extent. As the derangement of the inner aura progresses there occurs pare passu a change in the outer, which frequently can be verified by the chromatic alterations in the c.c. bands over the affected portions. Besides, the charging of the patient with static electricity will sometimes be of assistance in determining the true width of the inner aura, and consequently the extent of the derangement of the outer, as this proceeding causes the inner aura to vanish before the outer, leaving a void space. However, it is not always easy to decide whether there has been an increase of one of the auras at the expense of the other.
The following case affords a very good illustration of a similar change affecting both auras, making the inner aura appear widened; and of the separation of the two auras by the help of static electricity. There are, besides, other peculiarities which make the case worth quoting.
Case 69. (Fig. 54). I.W., a girl twenty years old was lately examined. Twelve months previously she had an attack of influenza complicated by pleurisy, on the left side, and subsequently she had undergone an operation for empyema. A few months later enlarged glands were removed from the right side
of her neck. When eleven years old she was a patient in the Hospital suffering from paralysis of both legs, and was discharged as incurable; but two days after reaching home she had suddenly regained the use of her legs.
When inspected both auras were normal in distinctness. The outer was spatulate
 Click to enlarge Fig. 54. Granular outer and inner auras. Void space by neck. |
patient standing on the insulated stool received a sufficiently large positive charge to cause the inner aura to vanish, but not enough to abolish the outer, the void space could be seen as nearly as possible of the same width as the inner aura in other places, viz, three inches, thus proving that the outer aura to a depth of three inches partook of the same granular alteration. With a larger charge it was noticed that the granular outer aura was the last to depart.
The c.c. band also presented some abnormalities. First of all the whole of the left side from the level of the clavicle downwards looked darker than on the right. This deepening of colour commenced in the middle of the spine at the back, and extended round to the front to about an inch to the left of the median line. As the girl stood facing, the right extension of the c.c. band was normal, while the left extension appeared darker, but it was difficult to obtain the true colour as the band was projected on to the aura itself on a plane in front of the trunk, and seemed to be mixed up with the granules. This was a unilateral instance of a phenomenon already mentioned. (Page 158). A dark spot was also discovered upon the nape of the neck.
To sum up, the inner aura does not vary in shape and size to the same extent as does the outer, and the chief morbid changes manifest themselves as alterations of substance. It is plain from the cases quoted, that variations in shape and size of the outer aura occur frequently and extensively, while in general structural modifications are either so slight or so delicate as to be almost imperceptible.
Nothing much can be said about the hue of an aura seen without a screen. The colours are for the most part limited to blue or grey, or to the mixtures of the two in different proportions. Temperament and mental powers seem to be of more importance in
this direction than are temporary changes in the health. In the following table compiled from the first hundred examinations made, auras have been classified according to their colours under the different headings. I. Blue auras. II. Blue mixed with grey auras. III. Grey auras. (N.B. The table originally published in the first edition of this book has been retained unaltered, as the overwhelming majority of the people examined since have been in ill-health).
|
I. |
Blue series. Forty cases. |
|
|
|
No individuals below, some above the average in mental power. |
|
|
II. |
Blue with more or less grey. Thirty-six cases. |
|
|
|
Some individuals below, none above the average in mental power. |
|
|
|
One case of hemiplegia. |
included in this class. |
|
|
Two epileptics. | |
|
|
One case of meningitis. | |
|
III. |
Grey series. Seventeen cases. |
|
|
|
All below the average in mental power. |
|
|
|
Two eccentric people. |
|
|
|
Six epileptics. |
included in this class. |
|
|
One case of general paralysis. | |
|
|
Three mentally dull. |
In the remaining seven cases no note was taken of the colour of the aura.
This table shows conclusively that the owners of blue auras are generally best endowed mentally.
A congenital grey aura indicates a deficiency of the intellectual faculties, but it has not been ascertained whether the loss of brain power through disease would change the colour of the aura to grey, which seems not unlikely.
N.B. It should be remembered that in all cases the colours of auras are faint and delicate.